Muscle action potentials (MAPs) are electrical responses recorded from muscles, indicating axonal connectivity and muscle fiber regeneration for voluntary contraction. This process is essential for understanding how muscles contract and generate force and movement. Skeletal muscles, for example, work with the bones of the skeleton to enable body movements, such as walking or swimming, and other functions like breathing and swallowing. The initiation and execution of skeletal muscle contractions occur when an action potential travels along a motor nerve to its endings on muscle fibers, causing the release of acetylcholine (ACh). This results in the opening of ACh-gated cation channels, allowing sodium ions to diffuse into the muscle fiber membrane, leading to depolarization and subsequent muscle contraction.
Explore related products

$132.52 $210.99





What You'll Learn
![]()
The role of motor units and muscle action potential (MAP)
In biology, a motor unit is a collection of a motor neuron and the skeletal muscle fibres it innervates, including the neuromuscular junctions between the neuron and the fibres. The number of muscle fibres in a motor unit varies depending on the function of the muscle. For instance, the muscles that act on the largest body masses have motor units that contain more muscle fibres, whereas smaller muscles contain fewer muscle fibres in each motor unit. Motor units are generally not all simultaneously active to prevent complete muscle fatigue. Instead, some motor units rest while others are active, facilitating longer muscle contractions.
Motor units are organised slightly differently in invertebrates. Each muscle has few motor units, and each muscle fibre is innervated by multiple neurons, including excitatory and inhibitory neurons. In contrast, vertebrates regulate the force of contraction of muscles by controlling the number of activated motor units.
The excitation-contraction coupling mechanism converts the action potentials in the muscle fibres into muscle fibre contraction. The action potentials at the muscle cell membrane surrounding the myofibrils travel into the T-tubules, which are responsible for propagating the action potential from the surface to the interior of the muscle fibre. When T-tubules become depolarised, their dihydropyridine receptors undergo a conformational change that mechanically interacts with the ryanodine receptors on the sarcoplasmic reticulum. This interaction opens the ryanodine receptors, causing Ca2+ to be released from the sarcoplasmic reticulum. The resulting increased intracellular Ca2+ attaches to troponin C of the troponin complex on the thin filaments.
Muscle action potential (MAP) is the electrical response recorded from a muscle that indicates axonal connectivity, occurring when motor units are activated. MAP recordings are less effective in assessing nerve regeneration in the early months following a plexus injury. The MAP and even some faint contraction may be generated by the artificial synchronisation, induced by the stimulator, of all the available motor units.
Dehydration's Impact: Sore Muscles and Joints
You may want to see also
Explore related products






![]()
Excitation-contraction coupling
ECC can be understood as the steps in a process of muscular contraction from action potential (excitation) to the power stroke (contraction). An action potential is an electrical event that occurs in the plasma membrane of skeletal muscle fibres. This electrical event triggers the release of calcium from the sarcoplasmic reticulum, which leads to contraction.
The action potentials at the muscle cell membrane surrounding the myofibrils travel into the T-tubules, which are responsible for propagating the action potential from the surface to the interior of the muscle fibre. T-tubules contain dihydropyridine receptors that are adjacent to the terminal cisternae of the sarcoplasmic reticulum of the muscle fibre. When T-tubules become depolarized, their dihydropyridine receptors undergo a conformational change that mechanically interacts with the ryanodine receptors on the sarcoplasmic reticulum. This interaction opens the ryanodine receptors, causing the release of calcium from the sarcoplasmic reticulum.
The resulting increase in intracellular calcium attaches to troponin C of the troponin complex on the thin filaments. The binding of calcium to troponin causes troponin to undergo a configurational change, removing tropomyosin from its blocking position on the actin filament. This allows for the cross-bridging cycle, which describes the cyclic events necessary for the generation of force or tension within the myosin heads during muscle contraction.
Muscle Twitching: Is Anxiety the Culprit?
You may want to see also
Explore related products






![]()
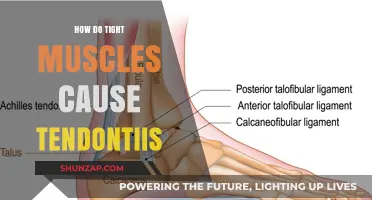
The function of T-tubules
T-tubules, or transverse tubules, are deep invaginations of the muscle cell membrane (sarcolemma) that penetrate the muscle fibre, or myofibril, which is the basic unit of the muscle fibre. They are responsible for propagating the action potential from the surface to the interior of the muscle fibre.
When an action potential reaches the T-tubules, it causes depolarisation, which leads to a conformational change in the T-tubules' dihydropyridine receptors. This mechanically interacts with the ryanodine receptors on the sarcoplasmic reticulum, opening them and causing the release of calcium ions (Ca2+) from the sarcoplasmic reticulum. This process is known as excitation-contraction coupling, which refers to the mechanism that converts the action potentials in the muscle fibres into muscle fibre contraction.
The released Ca2+ attaches to the troponin C of the troponin complex on the thin filaments, which are composed of actin, tropomyosin, and troponin. The troponin group comprises troponins I, T, and C and is located along the actin filaments next to tropomyosin. When calcium levels in the myocyte fall, the tropomyosin covers the actin filaments' myosin-binding sites, breaking the cross-bridge and causing muscle relaxation.
The T-tubular membranes are capable of passive electronic conduction of electrical changes in the surface membrane. They can also generate and propagate action potentials in response to surface membrane depolarisation. This enables the conduction of excitation into the depths of the muscle fibre, ensuring that the initiation of contractile activation is synchronised through the entire cross-section of the muscle fibre.
Facet Joint Injections: Unwanted Muscle Spasms?
You may want to see also
Explore related products






![]()
The importance of calcium (Ca2+)
Calcium ions (Ca2+) play a crucial role in the process of muscle contraction, specifically in the context of excitation-contraction coupling. This mechanism converts action potentials in muscle fibres into muscle fibre contraction.
The process begins with an action potential causing depolarisation in the myocyte membrane. This depolarisation spreads via transverse (T-tubules), which are invaginations of the muscle cell membrane. T-tubules are capable of passive electronic conduction of electrical changes in the surface membrane and can generate and propagate action potentials in response to surface membrane depolarisation. This ensures that the initiation of contractile activation is synchronised across the entire muscle fibre.
The depolarisation of T-tubules causes a conformational change in the dihydropyridine receptors, which mechanically interact with the ryanodine receptors on the sarcoplasmic reticulum. This interaction opens the ryanodine receptors, leading to the release of Ca2+ from the sarcoplasmic reticulum into the intracellular space.
The increase in intracellular Ca2+ ions is a critical step in muscle contraction. These ions attach to the troponin C component of the troponin complex on the thin filaments. This attachment leads to a series of structural changes that ultimately result in muscle contraction. The Ca2+ ions effectively activate the contractile elements, triggering the contraction process.
It is important to note that the calcium required for this process primarily comes from the internal stores of the sarcoplasmic reticulum rather than from external sources. This highlights the significance of intracellular calcium regulation in muscle contraction.
Dialysis and Muscle Pain: What's the Link?
You may want to see also
Explore related products






![]()
Voluntary vs involuntary contraction
Muscle contraction is a complex process that involves the interaction of various physiological components. At the most fundamental level, muscle contraction can be categorised into two types: voluntary and involuntary.
Voluntary muscle contraction is primarily associated with skeletal muscles, which are attached to bones and provide the body with structure and movement. These muscles are under the voluntary control of the somatic nervous system, allowing conscious control over movements such as facial expressions, swimming, or walking. The process of skeletal muscle contraction involves the propagation of action potentials along motor nerves, resulting in the release of acetylcholine (ACh) at the neuromuscular junction. ACh then acts on muscle fibres, causing the diffusion of sodium ions and subsequent depolarisation, which initiates another action potential and leads to muscle contraction.
In contrast, involuntary muscle contraction involves smooth and cardiac muscles, which are controlled by the autonomic nervous system. Smooth muscles are found in the internal organs, including the intestines, stomach, blood vessels, and uterus, and are responsible for pushing food through the digestive system and controlling blood vessel diameter. Cardiac muscles, on the other hand, comprise the walls of the heart and facilitate blood pumping. The contraction of cardiac muscles differs from skeletal muscles, as it involves electrical stimulation that releases calcium ions, leading to excitation-contraction.
Involuntary muscle contractions occur at regular intervals and are slower compared to voluntary contractions. As a result, involuntary muscles do not tire quickly and have lower energy requirements, hence possessing fewer mitochondria. Additionally, involuntary contractions can occur during specific scenarios, such as attempting to lift a weight that is too heavy, where the muscle involuntarily contracts to protect the joints from damage.
Understanding the intricacies of voluntary and involuntary muscle contraction is essential for comprehending the broader topic of how action potentials cause muscle contraction. The interplay between nerve impulses, chemical messengers, and ion movements ultimately leads to the complex process of muscle contraction, whether it be under voluntary or involuntary control.
Gemfibrozil's Muscular Pain: What You Need to Know
You may want to see also
Frequently asked questions
It is the electrical response recorded from a muscle that indicates axonal connectivity and occurs when motor units are activated.
T-tubules are responsible for propagating the action potential from the surface to the interior of the muscle fibre. They contain dihydropyridine receptors that, when depolarized, undergo a conformational change, interacting with the ryanodine receptors on the sarcoplasmic reticulum, causing the release of Ca2+.
An action potential travels along a motor nerve to its endings on muscle fibres. This causes the release of acetylcholine (ACh), which acts on the muscle fibre membrane to open ACh-gated cation channels. This allows sodium ions to diffuse into the muscle fibre, causing depolarization and initiating another action potential, leading to muscle contraction.
Skeletal muscle contraction is primarily voluntary and occurs in response to nerve impulses. In contrast, cardiac muscle has intrinsic spontaneous activity due to ion channels that cause depolarization. Skeletal muscle also lacks a substantial Ca2+ component in its action potential, unlike cardiac muscle.
Calcium ions (Ca2+) are released from the sarcoplasmic reticulum when ryanodine receptors open due to depolarization. The increased intracellular Ca2+ attaches to troponin C, initiating cross-bridge cycling and muscle contraction.