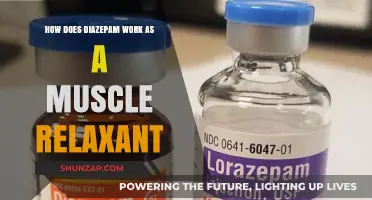
The digastric muscle, a unique bilateral muscle in the floor of the mouth, plays a crucial role in jaw movement and swallowing. Composed of two distinct bellies—an anterior belly originating from the mandible and a posterior belly attached to the temporal bone—it is connected by an intermediate tendon. When activated, the digastric muscle depresses the mandible, aiding in opening the mouth, while also assisting in elevating the hyoid bone during swallowing. Its dual-belly structure allows for coordinated action, making it essential for both mastication and speech, highlighting its significance in oral and pharyngeal functions.
| Characteristics | Values |
|---|---|
| Location | Anterior belly: Mandible (lower jaw) near the symphysis. Posterior belly: Hyoid bone and temporal bone (mastoid process). |
| Innervation | Anterior belly: Mylohyoid nerve (branch of the inferior alveolar nerve). Posterior belly: Facial nerve (cranial nerve VII). |
| Action | Opens the jaw (mandibular depression) when both bellies contract simultaneously. Assists in swallowing and speaking by stabilizing the hyoid bone. |
| Blood Supply | Anterior belly: Submental artery. Posterior belly: Occipital artery. |
| Unique Feature | Only muscle with dual innervation from different cranial nerves. |
Explore related products


$31.99 $39.99




What You'll Learn
- Origin and Insertion Points: Digastric muscle's anterior and posterior belly attachments to mandible and skull
- Nerve Supply: Controlled by mylohyoid nerve (anterior) and facial nerve (posterior) for coordinated movement
- Primary Function: Assists in opening the mouth by depressing the mandible during jaw movement
- Muscle Action: Works with other muscles to stabilize hyoid bone during swallowing and speech
- Clinical Significance: Digastric muscle dysfunction can cause jaw pain, trismus, or swallowing difficulties
![]()
Origin and Insertion Points: Digastric muscle's anterior and posterior belly attachments to mandible and skull
The digastric muscle, a unique bilateral muscle of the floor of the mouth, is a prime example of muscular duality, consisting of two distinct bellies—anterior and posterior—each with its own origin and insertion points. The anterior belly originates from the digastric fossa, a small depression on the inner surface of the mandible, just below the symphysis. This origin point is crucial for understanding the muscle's role in jaw movement, as it provides a stable base for the muscle's contraction. From here, the anterior belly inserts into the intermediate tendon, a fibrous band that connects the two bellies, acting as a bridge between the mandible and the skull.
In contrast, the posterior belly of the digastric muscle originates from the mastoid notch, a groove on the inferior surface of the skull's temporal bone. This origin is strategically positioned to allow the muscle to pull the mandible upward and backward during contraction. The posterior belly then inserts into the same intermediate tendon as the anterior belly, forming a functional unit that enables coordinated movement. This dual-origin structure is essential for the muscle's ability to depress the mandible and assist in opening the mouth, a fundamental action in speech, swallowing, and mastication.
To visualize the significance of these attachment points, consider the following analogy: the digastric muscle functions like a pair of tongs, with the anterior and posterior bellies acting as the arms and the intermediate tendon as the pivot point. When the muscle contracts, the tension created at the origin points—the digastric fossa and mastoid notch—is transferred through the tendon, causing the mandible to move in a controlled manner. This mechanism highlights the precision required in anatomical design to facilitate everyday activities.
Practical understanding of these origin and insertion points is vital in clinical settings, particularly in dentistry and oral surgery. For instance, during procedures involving the mandible or the floor of the mouth, knowledge of the digastric muscle's attachments helps in avoiding iatrogenic injuries. Additionally, in cases of temporomandibular joint (TMJ) disorders, assessing the function and integrity of these attachment points can provide insights into the underlying pathology. For students and practitioners, palpating the digastric fossa and mastoid notch during a physical examination can serve as a hands-on learning tool to reinforce anatomical knowledge.
In conclusion, the origin and insertion points of the digastric muscle’s anterior and posterior bellies are not merely anatomical landmarks but functional hubs that enable essential jaw movements. By understanding these attachments, one gains a deeper appreciation for the muscle’s role in daily activities and its clinical significance. Whether in education, practice, or research, this knowledge serves as a foundation for addressing musculoskeletal issues related to the mandible and skull.
Accelerate Muscle Relaxer Relief: Proven Tips for Quicker Results
You may want to see also
Explore related products






![]()
Nerve Supply: Controlled by mylohyoid nerve (anterior) and facial nerve (posterior) for coordinated movement
The digastric muscle, a unique bilateral muscle in the floor of the mouth, relies on a dual nerve supply for its precise and coordinated movements. This muscle, divided into anterior and posterior bellies, is innervated by two distinct nerves: the mylohyoid nerve and the facial nerve. Understanding this nerve supply is crucial for appreciating how the digastric muscle functions in activities like swallowing, speaking, and jaw movement.
Analytical Insight: The anterior belly of the digastric muscle is controlled by the mylohyoid nerve, a branch of the inferior alveolar nerve, which itself arises from the mandibular division of the trigeminal nerve (CN V3). This innervation ensures that the anterior belly works in tandem with the mylohyoid muscle, another key component of the oral floor. Together, they depress the mandible and elevate the hyoid bone during swallowing, a coordinated action essential for moving food from the mouth to the pharynx.
Instructive Guidance: To visualize this coordination, consider the act of swallowing. When you initiate a swallow, the mylohyoid nerve activates the anterior belly of the digastric muscle, while the facial nerve (CN VII) simultaneously activates the posterior belly. This dual activation ensures the hyoid bone and tongue move upward and forward, effectively pushing food into the pharynx. For clinicians or anatomy students, testing the integrity of these nerves can provide insights into neuromuscular health. For instance, weakness in the digastric muscle could indicate damage to either the mylohyoid or facial nerve, depending on the affected belly.
Comparative Perspective: Unlike other muscles in the head and neck, the digastric muscle’s dual nerve supply is a rare anatomical feature. Most muscles are innervated by a single nerve, but the digastric’s bifurcated control allows for finer motor coordination. This is particularly important given its role in delicate tasks like speech and swallowing. For example, the facial nerve’s involvement in the posterior belly highlights its broader role in facial expression and oral functions, while the mylohyoid nerve’s specificity underscores its focus on oral floor dynamics.
Practical Tips: For those studying or teaching anatomy, emphasizing the nerve supply of the digastric muscle can clarify its functional anatomy. Use diagrams or models to illustrate the pathways of the mylohyoid and facial nerves, and correlate this with clinical scenarios. For instance, a patient with facial nerve palsy might exhibit weakness in the posterior belly of the digastric muscle, leading to difficulty swallowing or altered speech. Understanding this relationship can aid in diagnosis and rehabilitation strategies, such as targeted exercises to strengthen the unaffected anterior belly.
Descriptive Takeaway: The digastric muscle’s nerve supply is a testament to the body’s intricate design. By dividing control between the mylohyoid and facial nerves, the muscle achieves a level of coordination that supports essential daily functions. This duality not only ensures efficient movement but also provides a diagnostic window into neurological health. Whether in the classroom, clinic, or research lab, appreciating this nerve supply enriches our understanding of how the digastric muscle works—and why it matters.
Effective Lower Chest Workout: Targeting Muscles for a Balanced Physique
You may want to see also
Explore related products






![]()
Primary Function: Assists in opening the mouth by depressing the mandible during jaw movement
The digastric muscle, a paired muscle located beneath the jaw, plays a pivotal role in the intricate mechanics of mouth opening. Its primary function is to assist in depressing the mandible, or lower jaw, during jaw movement, thereby facilitating the act of opening the mouth. This action is essential for various daily activities such as eating, speaking, and yawning. To understand its mechanism, consider the muscle's unique structure: it consists of two distinct bellies, the anterior and posterior, connected by a tendon that passes through the mandible. When the digastric muscle contracts, it pulls the mandible downward, counteracting the elevating forces of other muscles like the masseter and temporalis. This coordinated effort ensures smooth and controlled jaw movement.
From an anatomical perspective, the digastric muscle’s role in depressing the mandible is a prime example of neuromuscular coordination. The anterior belly, innervated by the mylohyoid nerve (a branch of the inferior alveolar nerve), and the posterior belly, innervated by the facial nerve, work in tandem despite their separate neural control. This dual innervation allows for precise modulation of force, ensuring the mandible lowers gradually rather than abruptly. For instance, during the initial phase of mouth opening, the digastric muscle activates subtly, while other muscles relax, demonstrating the body’s ability to fine-tune movements for efficiency and safety.
Practically, understanding the digastric muscle’s function is crucial for diagnosing and treating jaw-related disorders. For example, weakness or dysfunction in this muscle can lead to difficulties in fully opening the mouth, a condition known as trismus. Physical therapists often employ targeted exercises to strengthen the digastric muscle, such as gentle jaw stretches or resistance training using tools like therapy bands. Patients are typically instructed to perform these exercises 2–3 times daily, holding each stretch for 10–15 seconds to gradually improve muscle function. Early intervention can prevent complications like malnutrition or speech impairment in severe cases.
Comparatively, the digastric muscle’s role in jaw depression contrasts with the function of muscles like the masseter and temporalis, which primarily elevate the mandible during chewing. This antagonistic relationship highlights the balance required for proper jaw mechanics. While the masseter and temporalis generate powerful forces for mastication, the digastric muscle provides a counterforce that allows for controlled mouth opening. This dynamic interplay underscores the importance of muscular equilibrium in maintaining oral health and functionality.
Finally, a descriptive analysis of the digastric muscle’s action reveals its elegance in design. As the muscle contracts, the tendon connecting its two bellies acts as a pulley system, translating the force generated by the posterior belly into downward movement of the mandible. This mechanism is particularly efficient during activities like yawning, where a wide mouth opening is required. Observing this process in real-time, such as through medical imaging, can provide valuable insights into the muscle’s role and its potential vulnerabilities, guiding both therapeutic interventions and preventive care.
Creatine Phosphate: The Secret to Extended Muscle Endurance Explained
You may want to see also
Explore related products





![]()
Muscle Action: Works with other muscles to stabilize hyoid bone during swallowing and speech
The digastric muscle, a paired muscle located under the jaw, plays a crucial role in stabilizing the hyoid bone during swallowing and speech. This stabilization is not a solo act; it’s a collaborative effort involving other muscles, such as the geniohyoid, mylohyoid, and stylohyoid. Together, they form a dynamic system that ensures the hyoid bone remains steady, allowing for smooth and efficient oropharyngeal functions. Without this coordination, swallowing could become labored, and speech might lack clarity, highlighting the muscle’s indispensable role in daily activities.
To understand this action, consider the mechanics of swallowing. When you swallow, the digastric muscle contracts, pulling the hyoid bone upward and forward. Simultaneously, the geniohyoid and mylohyoid muscles contract to elevate the hyoid, while the stylohyoid provides additional support. This synchronized movement prevents the hyoid from shifting excessively, which could disrupt the closure of the pharynx and the passage of food into the esophagus. For individuals with weakened or imbalanced muscles, speech therapists often recommend targeted exercises, such as tongue presses or resisted jaw movements, to strengthen this coordination.
From a comparative perspective, the digastric muscle’s role in speech is equally fascinating. During speech, the hyoid bone acts as a pivot point for the tongue and larynx, influencing vowel and consonant production. The digastric muscle, along with its partners, ensures the hyoid remains stable, allowing for precise tongue and laryngeal movements. For instance, in producing the vowel /i/ (as in "see"), the hyoid elevates slightly, a movement facilitated by the digastric and mylohyoid muscles. Speech pathologists often emphasize the importance of maintaining muscle balance in this region to address articulation disorders, particularly in children aged 3–6, when speech development is most active.
A practical tip for enhancing digastric muscle function involves incorporating isometric exercises into daily routines. For example, gently pressing the tongue to the roof of the mouth for 10 seconds, repeated 5–10 times daily, can improve muscle tone. Additionally, avoiding prolonged jaw clenching or excessive gum chewing can prevent unnecessary strain on the digastric muscle. For older adults, who may experience muscle atrophy, gentle neck stretches and swallowing exercises prescribed by a therapist can help maintain hyoid stability and prevent dysphagia.
In conclusion, the digastric muscle’s collaboration with other muscles to stabilize the hyoid bone is a testament to the body’s intricate design. Whether in swallowing or speech, this coordination ensures seamless function, underscoring the importance of muscle health in everyday life. By understanding and supporting this system through targeted exercises and mindful habits, individuals can preserve the efficiency of these vital processes.
Stiff Leg Deadlift Muscles Worked: Targeted Benefits and Techniques
You may want to see also
Explore related products






![]()
Clinical Significance: Digastric muscle dysfunction can cause jaw pain, trismus, or swallowing difficulties
The digastric muscle, a paired muscle in the floor of the mouth, plays a pivotal role in jaw movement and swallowing. Its unique structure, divided into anterior and posterior bellies, allows it to depress the mandible and assist in opening the mouth. However, when dysfunction occurs, the consequences can be debilitating. Jaw pain, trismus (lockjaw), and swallowing difficulties are common symptoms that highlight the clinical significance of this muscle’s proper function. Understanding these issues is crucial for both patients and healthcare providers to address them effectively.
Consider a scenario where a patient presents with persistent jaw pain and difficulty opening their mouth. Upon examination, the digastric muscle may be identified as the culprit due to strain, inflammation, or nerve impingement. Trismus, often resulting from spasms or tightness in this muscle, can severely limit daily activities like eating or speaking. For instance, post-surgical patients or those with temporomandibular joint (TMJ) disorders frequently experience such symptoms. Early intervention, including physical therapy or anti-inflammatory medications, can prevent long-term complications.
Swallowing difficulties, or dysphagia, are another critical concern linked to digastric muscle dysfunction. This muscle’s posterior belly works in tandem with other muscles to elevate the hyoid bone and facilitate the swallowing reflex. When compromised, food or liquids may not pass smoothly into the esophagus, increasing the risk of aspiration pneumonia. Elderly patients or those recovering from stroke are particularly vulnerable. Speech therapists often employ exercises to strengthen the digastric muscle, such as jaw mobilization techniques or resistance training with therapy tools like jaw exercisers.
To mitigate these issues, a multidisciplinary approach is often necessary. Dentists, physical therapists, and otolaryngologists may collaborate to diagnose and treat digastric muscle dysfunction. For acute cases, warm compresses and gentle stretching can provide temporary relief. Chronic conditions might require botulinum toxin injections to relax overactive muscles or surgical intervention in severe cases. Patients should also be educated on lifestyle modifications, such as avoiding hard or chewy foods and practicing jaw relaxation exercises daily.
In summary, digastric muscle dysfunction is not merely a localized issue but a condition with far-reaching implications for oral and systemic health. Recognizing its role in jaw movement and swallowing underscores the importance of timely and targeted interventions. By addressing symptoms like jaw pain, trismus, and dysphagia proactively, individuals can maintain their quality of life and prevent complications. Whether through conservative management or advanced therapies, understanding this muscle’s clinical significance is key to effective treatment.
V-Sit Workout: Targeting Core Muscles for Strength and Stability
You may want to see also
Frequently asked questions
The digastric muscle is a small, paired muscle located in the floor of the mouth and under the jaw. It consists of two bellies: the anterior belly (attached to the mandible) and the posterior belly (attached to the hyoid bone and mastoid notch).
The digastric muscle assists in depressing the mandible (lowering the jaw) and stabilizing the hyoid bone during swallowing and speech. The anterior belly pulls the mandible downward, while the posterior belly helps elevate the hyoid bone.
Injury or dysfunction of the digastric muscle can lead to difficulty in opening the mouth, jaw pain, or issues with swallowing and speech. It may also cause asymmetry in jaw movement or discomfort during chewing.