Muscle quality is a broad term referring to muscle function, including force production, contraction, and relaxation. It is defined as the force generated per unit volume of muscle tissue. While muscle mass and muscle strength are often used as indicators of muscle quality, they do not always tell the full story. For example, a smaller muscle may be more effective than a larger one due to more contractile proteins, less fat infiltration, or other factors. Various methods can be used to assess muscle quality, including manual muscle testing, field testing, and dynamometry. However, there is no consensus on the optimal measure of muscle quality, and complex and expensive tests may not provide significantly better insights than simpler and less expensive tests such as grip strength. As new technologies emerge, the ability to measure muscle quality for individual muscles is becoming more feasible, but it is still largely measured for groups or regions of muscles.
| Characteristics | Values |
|---|---|
| Muscle quality definition | The force generated by each volumetric unit of muscle tissue |
| Muscle quality vs muscle mass | Muscle quality is a broad term referring to muscle function, including force production, contraction and relaxation, and metabolism. |
| Muscle quality and strength | Muscle quality did not outperform strength in tests. |
| Muscle quality and age | Aging is associated with decreases in muscle mass, muscle strength, and muscle power, with muscle strength declining at a higher rate than muscle mass. |
| Muscle quality and obesity | Obesity is a determining factor for functional decline. |
| Muscle quality and injury | Differences in muscle quality between sides of the body can lead to injury. |
| Muscle quality and contractile tissue | The more contractile tissue a muscle consists of, the stronger it is and the higher the muscle quality is. |
| Muscle quality measurement | There is no consensus on an optimal measure of muscle quality. Tests include manual muscle testing, field testing, dynamometry, and magnetic resonance imaging (MRI). |
Explore related products






What You'll Learn
![]()
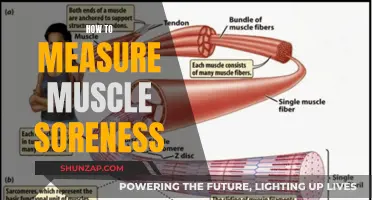
Muscle quality vs. muscle quantity
Muscle quality and muscle quantity are both important factors in clinical outcomes. Muscle quantity, or muscle mass, is the total skeletal muscle mass in the human body. It can be accurately determined using computed axial tomography (CT) and magnetic resonance imaging (MRI), but these methods are costly and not easily accessible. Other methods for determining muscle mass include bioelectrical impedance analysis (BIA) scales, which estimate body fat percentage, and circumference measurements, such as those used by the U.S. military. However, these methods are not as accurate as CT or MRI scans.
On the other hand, muscle quality refers to the capacity of a muscle to generate force and includes factors such as strength, power, endurance, and flexibility. Muscle quality is more challenging to define and measure than muscle quantity due to its complex nature. It involves the integration of functional and structural characteristics of the muscle, including the interaction of muscle fibres, fat infiltration, fibre type, and neural factors. While there are tests to determine muscle strength, such as manual muscle testing, field testing, and dynamometry, they often measure a group of muscles rather than a single muscle.
The relationship between muscle quantity and muscle quality is not fully understood. While greater muscle mass can generally produce greater muscle strength, it is not clear if higher muscle mass is associated with higher muscle quality. Some studies have found an inverse relationship between muscle mass and quality, suggesting that individuals with sarcopenia, a condition characterised by low muscle mass, may have better muscle quality than nonsarcopenic individuals. Additionally, muscle quality has been found to be more important than muscle quantity in predicting mortality, especially in older adults.
As new technologies and methods emerge, it is becoming easier to measure muscle quality for individual muscles. For example, magnetic resonance spectroscopy can quantify microscopic intramyocellular lipid droplets, and ultrasonography (US) can reflect muscle quantity and quality by measuring muscle thickness and echogenicity. Overall, while muscle quantity and muscle quality are both important, muscle quality is an emerging area of focus, especially in the context of ageing and clinical outcomes.
Heart Muscle and Oxygen: A Vital Relationship
You may want to see also
Explore related products






![]()
Muscle strength testing
The most commonly accepted method of evaluating muscle strength is the Medical Research Council Manual Muscle Testing scale. This method involves testing key muscles from the upper and lower extremities against the examiner's resistance and grading the patient's strength on a scale of 0 to 5. The test does not require any specialized equipment and is easy to perform. However, it also has some limitations, such as subjectivity in scoring based on the examiner's perception and variability in the maximal resistance that different examiners can apply.
Commonly tested muscles include the shoulder abductors, elbow flexors, elbow extensors, wrist extensors, finger flexors, hand intrinsics, hip flexors, knee extensors, dorsiflexors, great toe extensors, and plantar flexors. These muscle groups are chosen to assess important spinal nerve roots systematically. For example, testing the strength of the elbow flexors, elbow extensors, wrist extensors, finger flexors, and hand intrinsics can provide a methodical evaluation of the C5 to T1 nerve roots.
In addition to the Medical Research Council Manual Muscle Testing method, there are other ways to assess muscle strength, including the Oxford Scale and dynamometry. The Oxford Scale is commonly accepted and does not require special equipment, but it may not be applicable to all patients, as many patients assessed by physiotherapists do not possess a full range of motion due to their respective pathologies. Dynamometry, on the other hand, provides a more precise measurement of the force a muscle can exert and can track strength changes over time. However, a cross-sectional study showed a lower correlation between handgrip strength and standard strength measures of the lower limbs in older women.
How Bones and Muscles Work Together
You may want to see also
Explore related products






![]()
Manual muscle testing
During MMT, each muscle group is tested bilaterally. The examiner stands on the side of the patient being tested, and the patient is sitting upright and positioned to allow full movement of the joint against gravity. The examiner demonstrates the desired movement against gravity and then requests the patient to repeat the motion. If the patient can move through the desired range of motion against gravity, the examiner attempts to apply resistance in the testing position while giving instructions such as "Hold it, don't let me push it down" or "Hold it, don't let me bend it". The resistance is gradually increased until the patient's limit is found. The patient's strength is then graded on a scale from 0 to 5, with Grade 3 corresponding to "movement observed through a full range and test position held against gravity but not against moderate break force".
The most commonly accepted method of evaluating muscle strength is the Oxford Scale (aka Medical Research Council Manual Muscle Testing scale). This method involves testing key muscles from the upper and lower extremities against the examiner's resistance. Commonly tested muscles include the shoulder abductors, elbow flexors, elbow extensors, wrist extensors, finger flexors, hand intrinsic, hip flexors, knee extensors, dorsiflexors, great toe extensor, and plantar flexors.
MMT is a highly reliable method for assessing strength in patients following acute respiratory distress syndrome (ARDS) and other critical illnesses, as it can be completed with mechanically ventilated patients who can tolerate sitting upright in bed and follow two-step commands. It is also possible to modify the test for bedridden patients.
The Pectinate Muscle: A Small But Mighty Heart Helper
You may want to see also
Explore related products






![]()
Muscle quality and metabolic health
Muscle quality and muscle mass are important factors in clinical outcomes, with muscle strength being a widely used method for evaluating muscle quality. Muscle strength has been reported to be significantly associated with metabolic health, risk of cardiovascular events, and overall mortality.
Muscle quality is a broad term referring to muscle function, including force production, contraction and relaxation, and metabolism. It is quantified as muscle strength or intramuscular fat content. Measurement of muscle strength can be categorized into three types: manual muscle testing, field testing, and dynamometry. Manual muscle testing determines muscle strength through observation, palpation, and force application by an examiner, and strength is graded from 0 to 5. Field tests use body weight as a primary means of quantification for resistance and time, while dynamometry uses machines to measure muscle strength more accurately.
The most accurate way to calculate muscle mass percentage is to use magnetic resonance imaging (MRI). An MRI uses strong magnets to take images of your muscles by rearranging your body's hydrogen atoms and measuring the released energy. However, it is very expensive and not a practical choice for estimating muscle mass percentage. A more affordable option is to use a body fat scale that uses bioelectrical impedance to estimate body fat percentage. By inputting your height, weight, gender, and age, the scale can estimate your body fat percentage, and you can subtract this number from 100 to get your lean body mass percentage.
Studies have shown that dietary protein and leucine or its metabolite, β-hydroxy β-methylbutyrate (HMB), can improve muscle function and performance. Additionally, high-protein oral nutritional supplements (ONS) can help maintain and rebuild muscle mass and strength. Exercise, such as weight training and aerobic physical activities, also plays a crucial role in improving muscle mass and metabolic health.
Masturbation and Muscle Recovery: Any Benefits?
You may want to see also
Explore related products






![]()
Muscle quality and age
Muscle quality is a broad term referring to muscle function, including force production, contraction and relaxation, and metabolism. It is well-known that muscle strength declines with age, and this is associated with both mortality and physical disability. However, the loss of muscle strength is much more rapid than the loss of muscle mass, suggesting that a decline in muscle quality is also a factor in the strength decline.
The mechanisms determining muscle quality largely arise from neurological and skeletal muscle properties, as the output from these sources controls muscle force production. Within the neuromuscular system, several potential sites affect muscle quality, such as excitatory drive to the lower motor neurons, α-motor neuron excitability, neuromuscular transmission, and excitation–contraction (E–C) coupling. Age-related changes in spinal properties and the neuromuscular junction, such as decreased spinal excitability and a reduction in maximal motor unit discharge rates, may contribute to impairments in voluntary activation capacity and, thus, reduced muscle quality.
In addition, an increasing number of investigations report an age-related decline in autophagy. Autophagy is a process of cell and organelle degradation that also serves valuable housekeeping functions in normal, healthy cells by removing damaged or dysfunctional organelles. This latter function is often referred to as macroautophagy, and recent evidence suggests that this process is lost or impaired in ageing muscles. It is hypothesized that impaired autophagy leads to the accumulation of dysfunctional, damaged proteins, lipids, and nucleic acids that function at a suboptimal level. Dysfunctional contractile proteins, for example, might produce less force than normal and, thus, could contribute to impaired muscle quality.
Furthermore, obesity, but not low muscle mass, is a major determining factor for functional decline. Myosteatosis, which is excessive fat deposition in muscles, affects muscle quality. Aside from excessive energy intake, muscle injury, disuse, chronic inflammation, insulin resistance, mitochondrial dysfunction, defective leptin signaling, sex steroid deficiency, or increased glucocorticoid levels can also cause myosteatosis. Myosteatosis adversely affects not only muscle strength and mobility but also overall survival and prognosis related to underlying diseases.
Simple screening tools for sarcopenia and well-validated methods for assessing muscle mass and quality are available. Resistance training can prevent sarcopenia, and preventative diet, exercise, or treatment interventions, particularly in middle-aged adults, may help preserve mobility in later years and improve health spans.
First Muscle-Up: A Milestone in My Fitness Journey
You may want to see also
Frequently asked questions
Muscle quality is defined as the force generated per unit of volumetric muscle tissue. While there is no consensus on the best way to measure muscle quality, there are several methods that can be used, including manual muscle testing, field testing, and dynamometry. Dynamometry can be further divided into isokinetic dynamometry and handgrip dynamometry. Other methods include magnetic resonance imaging (MRI), computerized tomography (CT), and ultrasound.
Muscle quality is important because it can be used to predict clinical outcomes such as metabolic health, the risk of cardiovascular events, and overall mortality. It is also important because it can help explain age-related declines in muscle strength that cannot be attributed to decreases in muscle mass alone.
Muscle mass refers to the size of your muscles, whereas muscle quality refers to muscle function, including force production, contraction, and relaxation. While muscle mass and muscle strength are closely correlated, muscle quality is a more nuanced measure that takes into account factors such as the amount of contractile tissue, fat infiltration, and other physiological properties that can affect muscle strength.