The question of whether a sphincter muscle is open or closed when relaxed is a fundamental aspect of understanding its function in the human body. Sphincters are circular muscles that act as valves, controlling the passage of substances through various openings, such as the digestive and urinary systems. When relaxed, most sphincter muscles remain in a closed position, preventing the involuntary flow of materials. However, this default state can vary depending on the specific sphincter and its anatomical location. For instance, the internal anal sphincter is typically closed at rest, while the external anal sphincter can be consciously controlled. Exploring this topic sheds light on the intricate mechanisms that regulate bodily functions and highlights the importance of sphincter muscles in maintaining homeostasis.
| Characteristics | Values |
|---|---|
| Resting State | Closed when relaxed (most sphincters, e.g., esophageal, anal) |
| Exception | Internal anal sphincter remains open when relaxed |
| Function | Prevents unwanted passage of substances (e.g., food, waste) |
| Control | Involuntary (smooth muscle) or voluntary (striated muscle) |
| Examples of Closed-When-Relaxed | Esophageal sphincter, pyloric sphincter, anal sphincter (external) |
| Example of Open-When-Relaxed | Internal anal sphincter |
| Neural Regulation | Controlled by the autonomic nervous system (sympathetic/parasympathetic) |
| Clinical Significance | Dysfunction can lead to conditions like GERD, incontinence, or constipation |
Explore related products

$21.95 $27.95





What You'll Learn
- Resting State of Sphincters: Understanding if sphincter muscles are naturally open or closed when in a relaxed state
- Lower Esophageal Sphincter: Examining if the LES is open or closed during relaxation to prevent reflux
- Anal Sphincter Function: Investigating the default position of the anal sphincter when relaxed
- Urethral Sphincter Behavior: Analyzing if the urethral sphincter is open or closed at rest
- Pyloric Sphincter Relaxation: Determining the resting state of the pyloric sphincter in digestion
![]()
Resting State of Sphincters: Understanding if sphincter muscles are naturally open or closed when in a relaxed state
Sphincter muscles, by their very nature, are designed to control the passage of substances through various bodily orifices. Their resting state—whether open or closed when relaxed—varies depending on their location and function. For instance, the esophageal sphincter, which prevents stomach acid from flowing back into the esophagus, is typically closed at rest. This ensures that digestive acids remain where they belong, safeguarding the delicate lining of the esophagus. Conversely, the internal urethral sphincter, which controls the release of urine, is naturally closed when relaxed, maintaining continence without conscious effort. Understanding these differences is crucial for diagnosing and treating conditions like gastroesophageal reflux disease (GERD) or urinary incontinence.
Consider the anal sphincter, a muscle that exemplifies the complexity of sphincter behavior. It consists of two components: the internal sphincter, which is involuntary and remains closed at rest, and the external sphincter, which is under voluntary control. This dual mechanism ensures that waste is retained until the individual consciously decides to release it. Interestingly, the internal anal sphincter’s resting state is closed due to its smooth muscle composition, which is always tonically contracted. This design highlights the body’s prioritization of containment over release in certain areas, a principle that applies to other sphincters like the pyloric sphincter, which regulates stomach emptying into the small intestine.
To illustrate further, the pupillary sphincter in the eye provides a unique contrast. Unlike digestive or urinary sphincters, it controls the size of the pupil in response to light. In a relaxed state, the pupillary sphincter is open, allowing more light to enter in dim conditions. However, when exposed to bright light, it contracts to reduce the pupil size, demonstrating how environmental factors can override the resting state. This example underscores the diversity of sphincter functions and how their resting states are tailored to their specific roles.
Practical implications of understanding sphincter resting states extend to medical interventions and lifestyle adjustments. For instance, individuals with GERD may benefit from medications that enhance the lower esophageal sphincter’s tone, keeping it closed more effectively. Similarly, pelvic floor exercises can strengthen the external anal sphincter, improving control for those with incontinence. For the pupillary sphincter, wearing sunglasses in bright light can reduce strain by minimizing the need for constant contraction. These targeted approaches highlight the importance of recognizing and respecting the natural resting states of sphincters in maintaining bodily function.
In conclusion, the resting state of sphincters—whether open or closed—is not a one-size-fits-all concept. It is dictated by their anatomical location, physiological role, and the body’s need for containment or release. By understanding these nuances, healthcare providers and individuals can better address disorders related to sphincter dysfunction. Whether through medication, exercise, or environmental modifications, respecting the natural tendencies of these muscles is key to optimizing their function and overall well-being.
Citalopram and Muscle Relaxation: Exploring Its Effects on Tension Relief
You may want to see also
Explore related products






![]()
Lower Esophageal Sphincter: Examining if the LES is open or closed during relaxation to prevent reflux
The lower esophageal sphincter (LES) is a critical gatekeeper between the esophagus and stomach, but its behavior during relaxation is often misunderstood. Unlike some sphincters that remain closed at rest, the LES is tonically contracted, meaning it stays closed when relaxed to prevent stomach acid from flowing back into the esophagus. This baseline closure is essential for maintaining digestive health and preventing gastroesophageal reflux disease (GERD). However, certain factors—such as overeating, lying down immediately after meals, or consuming trigger foods like caffeine or alcohol—can weaken this closure, allowing acid to escape. Understanding this mechanism is key to managing reflux symptoms effectively.
To examine the LES’s role in reflux prevention, consider its physiological function during digestion. When food approaches the stomach, the LES temporarily opens to allow passage, then promptly closes to seal the stomach’s contents. This process is regulated by neural and hormonal signals, ensuring the sphincter remains closed except during swallowing. However, in individuals with GERD, the LES may relax inappropriately or fail to close completely, leading to chronic acid reflux. For example, studies show that transient LES relaxations (TLESRs) account for up to 90% of reflux episodes in GERD patients, highlighting the importance of maintaining proper LES function.
Practical strategies to support LES integrity include lifestyle modifications and dietary adjustments. Elevating the head of the bed by 6–8 inches can reduce nighttime reflux by using gravity to keep acid down. Avoiding large meals, especially within 2–3 hours of bedtime, minimizes pressure on the LES. Additionally, limiting known irritants like spicy foods, citrus, and carbonated beverages can decrease the likelihood of sphincter relaxation. For persistent symptoms, medications such as proton pump inhibitors (e.g., omeprazole 20–40 mg daily) or H2 blockers (e.g., ranitidine 150 mg twice daily) may be prescribed to reduce acid production and alleviate strain on the LES.
Comparing the LES to other sphincters, such as the anal or urinary sphincters, reveals distinct differences in function and control. While the anal sphincter is voluntarily controlled and relaxed at rest, the LES operates involuntarily and remains contracted unless triggered to open. This distinction underscores the LES’s unique role in preventing reflux, as its failure to maintain closure—even briefly—can have significant health implications. For instance, prolonged LES dysfunction can lead to esophageal damage, Barrett’s esophagus, or even esophageal cancer, making early intervention crucial.
In conclusion, the LES is closed during relaxation to prevent reflux, but its effectiveness depends on various factors, from dietary choices to anatomical integrity. By understanding its function and implementing targeted interventions, individuals can mitigate reflux symptoms and protect their digestive health. Whether through lifestyle changes, medication, or medical advice, addressing LES dysfunction is a proactive step toward long-term wellness.
Is Xanax a Muscle Relaxer? Prescription Frequency and Uses Explained
You may want to see also
Explore related products






![]()
Anal Sphincter Function: Investigating the default position of the anal sphincter when relaxed
The anal sphincter, a critical component of the human digestive system, operates with a default state that is inherently closed when relaxed. This involuntary muscle, composed of both internal and external components, is designed to maintain continence by sealing the anal canal. The internal sphincter, controlled by the autonomic nervous system, remains contracted without conscious effort, ensuring that fecal matter is retained until deliberate release is initiated. This baseline closure is essential for preventing accidental soiling, particularly during sleep or periods of inattention.
Understanding the relaxed state of the anal sphincter requires a comparative analysis of its structure and function. Unlike other sphincters, such as the esophageal or urinary sphincters, which may exhibit variability in their default positions, the anal sphincter’s closed state is non-negotiable for hygiene and social functionality. The external sphincter, under voluntary control, complements the internal sphincter by providing additional closure when needed. However, even when the external sphincter is consciously relaxed, the internal sphincter’s tonic contraction ensures the anal canal remains sealed, highlighting its primary role in continence.
From a practical standpoint, disruptions to the anal sphincter’s default closed position can lead to significant health issues, such as fecal incontinence. Conditions like sphincter injury, neurological disorders, or aging can impair its function, necessitating interventions like Kegel exercises, biofeedback therapy, or surgical repair. For instance, individuals over 65 are more prone to sphincter weakening due to muscle atrophy, making targeted strengthening exercises particularly beneficial for this age group. Incorporating dietary fiber (25–30 grams daily) and adequate hydration can also support stool consistency, reducing strain on the sphincter.
A persuasive argument for prioritizing anal sphincter health lies in its impact on quality of life. The embarrassment and social isolation associated with incontinence underscore the importance of maintaining its default closed state. Proactive measures, such as avoiding chronic constipation through regular physical activity and mindful toilet habits (e.g., not straining during bowel movements), can preserve sphincter integrity. For those with existing issues, consulting a gastroenterologist or pelvic floor specialist is crucial for tailored treatment plans, which may include medications like antidiarrheals or muscle relaxants, depending on the underlying cause.
In conclusion, the anal sphincter’s default position when relaxed is unequivocally closed, a design feature vital for human dignity and hygiene. Its dual-component structure—involuntary internal and voluntary external—ensures robust continence under normal circumstances. Recognizing the factors that compromise this function and adopting preventive strategies can mitigate risks, particularly in vulnerable populations. By treating the anal sphincter with the attention it deserves, individuals can safeguard their health and maintain a higher standard of living.
Understanding Muscle Cell Relaxation: Mechanisms and Key Processes Explained
You may want to see also
Explore related products






![]()
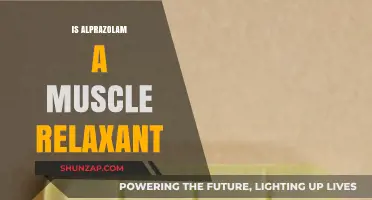
Urethral Sphincter Behavior: Analyzing if the urethral sphincter is open or closed at rest
The urethral sphincter, a critical component of urinary continence, exhibits a unique behavior at rest that is essential to understand for both medical professionals and individuals seeking to comprehend their body’s functions. Unlike some sphincters, such as the lower esophageal sphincter, which remains closed when relaxed to prevent reflux, the urethral sphincter operates under a different principle. At rest, the external urethral sphincter, composed of voluntary skeletal muscle, is typically in a state of mild contraction, maintaining closure to prevent involuntary urine leakage. This voluntary control distinguishes it from the internal urethral sphincter, which is involuntary and remains tonically contracted due to sympathetic nervous system activity.
Analyzing this behavior requires a deeper look at the physiological mechanisms at play. The external urethral sphincter’s resting state is influenced by the pudendal nerve, which innervates the muscle and allows for conscious control. When relaxed, this sphincter does not fully open but rather maintains a baseline tone to ensure continence. In contrast, the internal urethral sphincter, part of the bladder neck, remains closed at rest due to alpha-adrenergic stimulation, ensuring urine is retained in the bladder until deliberate voiding occurs. This dual system highlights the body’s intricate design to balance voluntary and involuntary control.
Practical implications of this behavior are significant, particularly in diagnosing and treating conditions like stress incontinence or urinary retention. For instance, in older adults or individuals with neurological disorders, weakened voluntary control of the external urethral sphincter can lead to leakage during activities like coughing or sneezing. Conversely, overactivity of the internal sphincter or bladder neck can cause difficulty initiating urination. Understanding the resting state of these sphincters aids in targeted interventions, such as pelvic floor exercises (Kegel exercises) to strengthen the external sphincter or alpha-blocker medications (e.g., tamsulosin 0.4 mg daily) to relax the internal sphincter in cases of benign prostatic hyperplasia.
A comparative analysis with other sphincters underscores the urethral sphincter’s unique role. While the anal sphincter also relies on voluntary control at rest, its involuntary component (the internal anal sphincter) is regulated by the enteric nervous system, differing from the urethral sphincter’s sympathetic control. This distinction highlights the importance of context-specific understanding when addressing sphincter-related issues. For example, pelvic floor physical therapy may benefit both urethral and anal sphincter dysfunction but requires tailored approaches based on their distinct neural and muscular characteristics.
In conclusion, the urethral sphincter’s behavior at rest is a delicate balance of voluntary and involuntary mechanisms, with the external sphincter maintaining mild contraction for continence and the internal sphincter remaining closed via sympathetic activity. This knowledge is pivotal for addressing urinary disorders and underscores the need for personalized treatment strategies. Whether through behavioral modifications, pharmacotherapy, or physical therapy, understanding this resting state empowers both healthcare providers and individuals to manage urinary health effectively.
Effective Techniques to Release and Relax Your Tight Psoas Major Muscle
You may want to see also
Explore related products






![]()
Pyloric Sphincter Relaxation: Determining the resting state of the pyloric sphincter in digestion
The pyloric sphincter, a crucial gatekeeper between the stomach and the small intestine, operates in a state of dynamic tension, balancing the need for controlled passage of chyme with the necessity of preventing backflow. Unlike some sphincters that remain closed at rest, the pyloric sphincter exhibits a unique behavior: it is tonically contracted in its resting state, yet this contraction is not absolute. This baseline tension ensures a regulated flow of partially digested food into the duodenum, preventing sudden surges that could overwhelm the intestine. Understanding this resting state is essential for diagnosing and treating disorders like pyloric stenosis or gastroparesis, where the sphincter’s function is compromised.
Analyzing the pyloric sphincter’s relaxation requires a closer look at its physiological triggers. During digestion, hormonal signals such as gastrin and neural inputs from the enteric nervous system modulate its tone. For instance, the presence of acidic chyme in the duodenum stimulates the release of secretin, which indirectly promotes pyloric relaxation to slow gastric emptying. Conversely, high fat content in the stomach delays relaxation, ensuring thorough mixing and digestion. This interplay highlights the sphincter’s responsiveness to luminal contents, making it a finely tuned regulator rather than a simple on-off valve.
From a practical standpoint, assessing pyloric sphincter function often involves imaging studies like ultrasound or barium contrast X-rays, particularly in pediatric cases of suspected pyloric stenosis. For adults, manometry—a procedure measuring pressure changes in the digestive tract—can provide direct insights into the sphincter’s resting tone and response to stimuli. Clinicians may also consider dietary modifications, such as smaller, more frequent meals, to manage conditions exacerbated by abnormal pyloric function. For severe cases, surgical intervention, such as pyloromyotomy, may be necessary to alleviate obstruction.
Comparatively, the pyloric sphincter’s resting state contrasts with other sphincters like the lower esophageal sphincter (LES), which is closed at rest to prevent acid reflux. This distinction underscores the pyloric sphincter’s role as a modulator rather than a barrier. While the LES relies on a high-pressure zone to maintain closure, the pyloric sphincter’s tonic contraction is more flexible, allowing gradual passage of chyme. This comparative analysis emphasizes the importance of context in understanding sphincter physiology and its implications for digestive health.
In conclusion, the pyloric sphincter’s resting state is one of tonic contraction, a nuanced balance that ensures controlled gastric emptying. Its responsiveness to hormonal and neural cues underscores its role as a dynamic regulator of digestion. By understanding this unique behavior, healthcare providers can better diagnose and manage disorders related to pyloric function, offering targeted interventions that restore digestive harmony. Whether through imaging, manometry, or dietary adjustments, addressing the pyloric sphincter’s resting state is key to optimizing gastrointestinal health.
Master Muscle Relaxation: Techniques for Stress Relief and Recovery
You may want to see also
Frequently asked questions
A sphincter muscle is typically closed when relaxed. Sphincters are circular muscles that constrict a passage or opening, and their natural state is to remain closed until they are actively contracted to open.
When a sphincter muscle contracts, it opens the passage or orifice it controls. This allows for the passage of substances, such as food, waste, or fluids, through the opening.
Yes, most sphincter muscles, such as the anal sphincter or esophageal sphincter, are closed when relaxed. However, some sphincters, like the pupillary sphincter in the eye, function differently and constrict (close) when contracted rather than when relaxed.