The anus is surrounded by a group of muscles called the anal sphincter, which controls the release of stool. The anal sphincter is made up of two muscles: the internal anal sphincter and the external anal sphincter, which work together to maintain faecal continence. The external anal sphincter is a skeletal muscle with a complex structure, composed of three parts that loop around the anal canal. The internal anal sphincter is located inside the rectum, while the external anal sphincter surrounds the end of the anal canal. These muscles can be affected by various conditions, such as anismus, anal fissures, and Crohn's disease, which can lead to faecal incontinence and other issues.
| Characteristics | Values |
|---|---|
| Definition | The anal sphincter is a group of muscles at the end of the rectum that surrounds the anus and controls the release of stool. |
| Location | The anal sphincter is located at the last few inches of the large intestine (colon). |
| Types | Internal anal sphincter, External anal sphincter |
| Composition | The external anal sphincter is made up of striated fibres and has a complex morphology. It is composed of three parts that loop around the anal canal: upper or deep, middle or superficial, and lower or subcutaneous. |
| Functions | The anal sphincter muscles regulate defecation and maintain faecal continence. |
| Disorders | Anismus, Anal fissures, Abscesses, Hemorrhoids, Faecal incontinence |
| Treatments | Pelvic floor exercises, Botox injections, Topical medications, Surgery |
Explore related products






What You'll Learn
![]()
The anal sphincter is a group of muscles at the end of the rectum
The anal sphincter is indeed a group of muscles located at the end of the rectum. The rectum is found at the end of the large intestine (colon), and the anal sphincter surrounds the anus, controlling the release of stool and maintaining continence. The anal sphincter is made up of two muscles: the internal anal sphincter and the external anal sphincter. These muscles work together to regulate defecation and maintain faecal continence.
The internal anal sphincter is located inside the rectum, while the external anal sphincter wraps around the outside of the end of the anal canal. The external anal sphincter is a complex skeletal muscle with a unique morphology. It is composed of three parts that loop around the anal canal: the upper or deep part, the middle or superficial part, and the lower or subcutaneous part. The middle part forms the main bulk of the muscle, attaching anteriorly and posteriorly to the anus within the perineal body and the anococcygeal ligament.
The anal sphincter muscles can be affected by various conditions. For example, anismus is a functional disorder of the pelvic floor muscles, including the external anal sphincter, caused by abnormal contractions during defecation. Anal fissures, tears in the lining of the anus, can also extend into the internal anal sphincter, causing pain and other symptoms. In addition, hemorrhoids, swollen veins around the anus, can occur above or below the internal and external anal sphincters, respectively, and may require medical treatment or surgery in severe cases.
Damage to the anal sphincter muscles can result in faecal incontinence, the involuntary release of stool. This can be caused by trauma to the anal sphincter, chronic diseases, neurological disorders, or inflammatory bowel disease. Diagnosis of anal sphincter disorders involves a physical examination, including a digital rectal examination, where a physician inserts a lubricated finger into the anus to check for tension, bleeding, and tenderness.
Muscle Mystery: Water Content and Muscular Performance
You may want to see also
Explore related products




$27.49 $29.95


![]()
The internal and external anal sphincters
The anus is surrounded by a group of muscles known as the anal sphincter, which is made up of two muscles: the internal anal sphincter and the external anal sphincter. These muscles work together to control the release of stool and maintain continence.
The internal anal sphincter is a smooth muscle that is located inside the rectum. It receives visceral innervation from sympathetic and parasympathetic fibres. It contracts to close the anal canal and prevent the passage of faeces, and it relaxes to allow the passage of faeces. The internal anal sphincter is not under voluntary control.
The external anal sphincter is a skeletal muscle made up of striated fibres. It is located at the intersection of many intricate muscle fibres and surrounds the outside of the end of the anal canal. It is under voluntary control, allowing it to stay in a contracted state to prevent defecation until the appropriate time. It is aided in this function by the sling-like puboanalis muscle, one of the levator ani muscles. The external anal sphincter also has a complex origin and insertion, as it does not follow the typical attachment pattern.
Several diseases, conditions, and injuries can affect the anal sphincters. For example, anismus is a functional disorder of the pelvic floor muscles, including the external anal sphincter, caused by a problem with the way these muscles contract and relax during defecation. Anal fissures are tears in the lining of the anus that often extend into the internal anal sphincter. They are caused by passing a very hard or large bowel movement and can become chronic. Hemorrhoids, which are swollen veins around the anus, can also be internal or external to the sphincters. In addition, people with Crohn's disease may develop problems in the anal sphincter, such as abscesses and inflammation.
Massaging Your Psoas Muscle: Techniques for Relaxation and Relief
You may want to see also
Explore related products






![]()
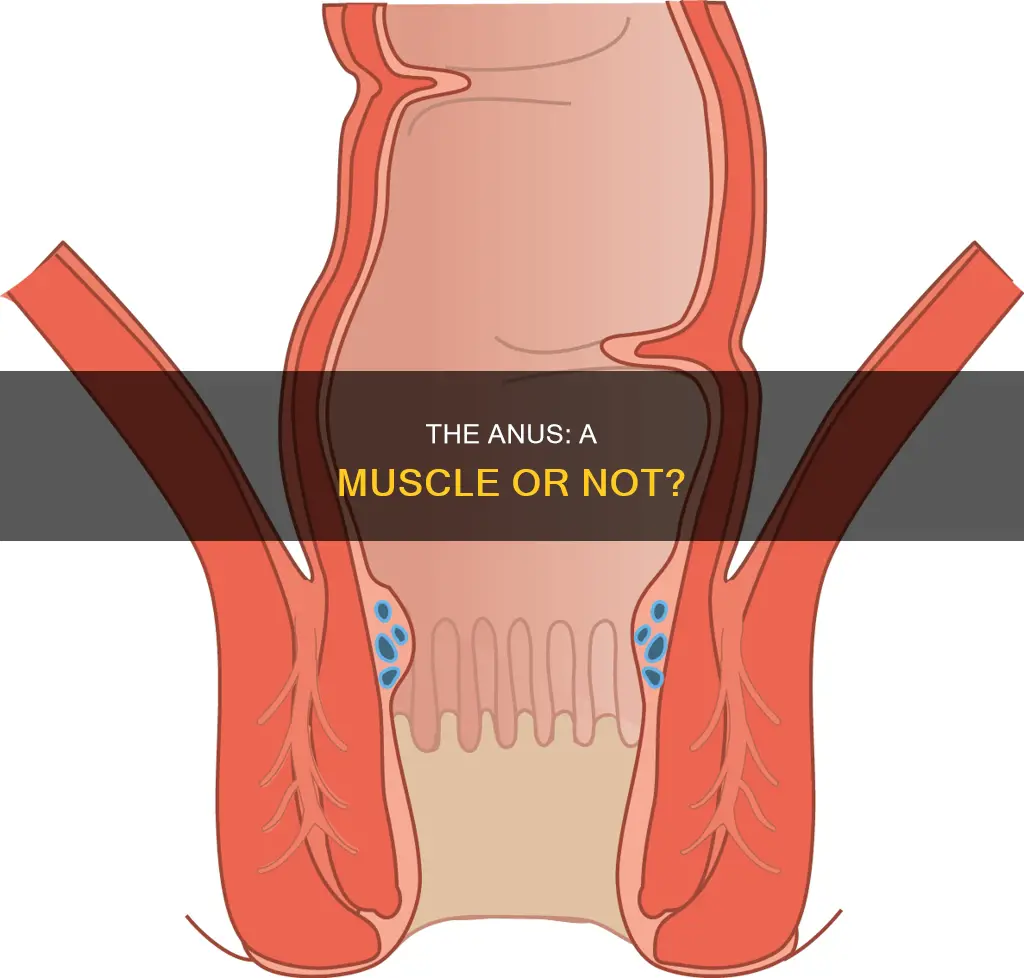
Anal fissures and how they are treated
The anus is surrounded by a group of muscles called the anal sphincter, which controls the release of stool. Anal fissures are small, painful tears in the lining of the anus, which can cause anal pain and rectal bleeding during bowel movements. They are usually caused by overstretching the anal canal, which can occur when passing very hard or large bowel movements.
Anal fissures are common, especially in infants, pregnant women, and people with constipation. They are often acute, meaning they heal within 6 weeks with minimal treatment. However, some fissures are more complicated and may resist healing, becoming chronic. Chronic anal fissures are those that have lasted more than 8 weeks and require more aggressive treatment.
Treatment for anal fissures typically focuses on relaxing the anal sphincter muscles, which allows the fissure to close and helps restore blood flow to the tissues. Bulk-forming laxatives are often prescribed to help retain fluid in the stool, making it softer and less likely to cause further tearing. Topical treatments such as GTN ointment, calcium channel blockers, and lidocaine can also be used to relax the sphincter muscle and increase blood flow to the fissure. Sitz baths, which are shallow warm water baths, can also help to relieve symptoms and relax the muscles.
In some cases, more invasive treatments may be necessary. Botulinum toxin (Botox) injections can be used to paralyse the sphincter muscle and prevent muscle spasms. Surgery may also be an option for chronic fissures that have failed to respond to other treatments.
Myoglobin and Muscles: What's the Rich Connection?
You may want to see also
Explore related products





![]()
Anismus and pelvic floor exercises
The anus is a group of muscles at the end of the rectum. The anal sphincter surrounds the anus and controls the release of stool. There are two types of anal sphincter muscles: the internal anal sphincter and the external anal sphincter.
Anismus, also known as pelvic floor hypertonicity, anal sphincter dysserynergia, dyssynergic defecation, and paradoxical puborectalis dysfunction, is a disorder of the external anal sphincter and puborectalis muscles (one of the pelvic floor muscles) during attempted bowel movements. It is a form of pelvic floor muscle dysfunction. During defecation, the pelvic floor muscles typically relax to allow for the evacuation of stool. However, with anismus, the puborectalis muscle and anal sphincter contract, preventing the stool from passing through the anal opening. This can result in painful and challenging obstructive constipation, fecal impaction, and an enlargement of the rectum called megarectum. Those with anismus may chronically bear down or strain in an attempt to have a bowel movement, further irritating the pelvic floor muscles.
Anismus is a treatable condition, and pelvic floor physical therapy can significantly improve symptoms and restore normal bowel function. The first step in treatment involves a detailed discussion of symptoms, medical history, and goals, followed by a comprehensive assessment of pelvic floor muscle function. Pelvic nerve tests and surface EMG biofeedback of the pelvic floor muscles assist in determining the severity of the spasm or hypertonicity and the possibility of normal relaxation of the pelvic floor muscles. This information is crucial for resolving anismus.
Treatment for anismus may include a combination of manual techniques, soft tissue mobilization, stretching exercises, visceral manipulation, neuromuscular re-education of the pelvic floor muscles, surface EMG biofeedback training, therapeutic exercises, and a home exercise program. Pelvic floor exercises are often recommended to treat anismus, and injections of Botulinum toxin (Botox) can also help. Maintaining the strategies and exercises learned during treatment is essential for preventing the recurrence of anismus.
Muscle Homeostasis: The Intricate Balance of Human Physique
You may want to see also
Explore related products






![]()
Faecal incontinence and its risk factors
The anus is part of the body's excretory system and is surrounded by a group of muscles called the anal sphincter, which controls the release of stool and maintains continence. Faecal incontinence is a condition where liquid or solid stool leaks out unintentionally. It can range from mild leakage when passing gas to severe cases of passing solid stools.
There are several risk factors associated with faecal incontinence. One significant factor is childbirth, particularly vaginal delivery, which can cause injuries to the anal sphincters and impair the continence mechanism. This is evident in studies where a substantial number of females attributed their symptoms of faecal incontinence to childbirth. Additionally, medical procedures involving the anal or rectal regions, such as surgery to remove haemorrhoids or treat abscesses, can lead to muscle and nerve damage, increasing the risk of faecal incontinence.
Age is another factor, with individuals over 65 being more susceptible to faecal incontinence due to the natural weakening of muscles with age. Sex also plays a role, with females having a higher risk, possibly due to experiences such as vaginal childbirth and hormone therapy for menopause. Certain conditions, such as neurologic diseases, inflammatory bowel disease, and haemorrhoids, can also increase the chances of faecal incontinence by affecting nerves, muscles, or tissue in the pelvic region.
Furthermore, diarrhoea and constipation are common risk factors for faecal incontinence. Diarrhoea fills the rectum quickly, making it harder to control, while constipation can lead to a large amount of stool in the rectum, causing chronic relaxation of the internal anal sphincters and allowing stool to seep out. It is important to note that individuals experiencing faecal incontinence should seek medical advice, especially if it affects their quality of life or causes emotional distress.
Organs and Muscles: What's the Connection?
You may want to see also
Frequently asked questions
The anus is the opening at the end of the rectum, which is located at the end of the large intestine (colon).
The anus is surrounded by a group of muscles called the anal sphincter, which controls the release of stool. The anal sphincter is made up of two muscles: the internal anal sphincter and the external anal sphincter.
The anal sphincter regulates defecation by maintaining faecal continence. It works to control the release of stool by opening and closing the anal canal.
Some common issues with the anal sphincter include anismus, anal fissures, haemorrhoids, and faecal incontinence. Anismus is a functional disorder of the pelvic floor muscles, including the external anal sphincter, which affects the way these muscles contract and relax during defecation. Anal fissures are tears in the lining of the anus, which can be caused by passing a very hard or large bowel movement. Haemorrhoids are swollen veins around the anus, which can be internal or external and may become trapped by the internal anal sphincter, causing pain. Faecal incontinence is the involuntary passage of stool due to rectal pressure exceeding anal sphincter pressure.