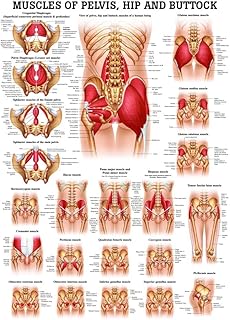
The psoas muscle is located in the retroperitoneal space, which is a complex anatomical area behind the peritoneal cavity and bordered by large muscles such as the diaphragm, abdominal wall, and paraspinous muscles. The retroperitoneum is not considered a true compartment due to the absence of distinct anatomical boundaries, but natural barriers to tumour spread exist, such as the fascia of the psoas muscle, which aid in defining the surgical space. The psoas muscle can be accessed through a retroperitoneal approach, which has been used to successfully treat tumours such as retroperitoneal neurofibroma and schwannoma.
| Characteristics | Values |
|---|---|
| Resection of the psoas muscle | Improved the quality of the excision |
| Caused little morbidity (denervation weakness of the quadriceps and anterior high numbness) | |
| Included resection of the femoral nerve, genitofemoral and ilioinguinal nerves | |
| Schwannoma in the psoas muscle | Removed by the retroperitoneal approach |
| Retroperitoneal surgery | Includes the psoas muscle, colon, kidney, and adrenal gland |
| Is a marginal resection |
Explore related products





What You'll Learn
![]()
Retroperitoneal cancer and the psoas muscle
Retroperitoneal cancer is a rare form of cancer that arises from mesenchymal cells and is usually located in muscle, fat, and connective tissues. The psoas muscle is indeed retroperitoneal, and cancer affecting this muscle is an uncommon condition called Malignant Psoas Syndrome (MPS). MPS is caused by malignant infiltration of the psoas muscle and adjacent nerves, resulting in fixed flexion deformity of the ipsilateral hip and proximal lumbosacral plexopathy.
Treatment options for retroperitoneal cancer involving the psoas muscle include surgery, radiotherapy, and chemotherapy. Surgery is often challenging due to the location of the tumour, and clear margins are difficult to achieve. Radiotherapy is sometimes used pre-operatively as it may provide the highest chance of safe and successful multimodal therapy. However, the poor prognosis of sarcoma in this region is due to delayed diagnosis and the tumour's proximity to vital structures.
In some cases, retroperitoneal tumours with psoas infiltration are treated with surgical resection of the psoas muscle, including the femoral nerve and other adjacent nerves. This procedure has been shown to cause minimal morbidity and improve the quality of the excision. In addition, ablation of the psoas muscle is technically possible and may enhance the patient's outlook for both palliation and curative intent.
Computed tomography (CT) and magnetic resonance imaging (MRI) scans are useful tools for assessing the extent of the tumour and planning the appropriate treatment approach. These imaging techniques help visualise the size and location of the tumour, as well as any displacement of adjacent structures, such as the kidney, bowel loops, and inferior vena cava.
Elliptical Training: Muscle Toning and Fitness
You may want to see also
Explore related products






![]()
Resection of the psoas muscle
The psoas muscle is a long, ribbon-shaped muscle that runs from the lower back to the groin. It is responsible for various functions, including moving the hips and upper legs, and supporting posture.
In certain cases, resection of the psoas muscle may be necessary. Resection refers to the surgical removal of a part of the body, in this case, the psoas muscle. This procedure is typically performed in cases of extensive retroperitoneal cancer or tumours within the psoas muscle. The resection of the psoas muscle can also include the removal of the femoral nerve and other surrounding nerves.
One case study describes a 16-year-old boy who presented with paresthesias and weakness in the right thigh. A tumour was identified within the right psoas muscle, which did not respond to chemotherapy. The patient underwent an anatomic resection of the psoas muscle and femoral nerve, followed by radiotherapy.
Another case study mentions three patients with extensive retroperitoneal cancer who underwent resection of the psoas muscle as part of a radical tumour excision. The procedure caused minimal morbidity and improved the quality of the excision.
It is important to note that psoas injuries are rare, and resection of the psoas muscle is a complex surgical procedure that should only be performed by specialised healthcare professionals.
Attract a Muscle Bear: Tips for Success
You may want to see also
Explore related products



![Psoas Release Tool - 3-in-1 Massage Tool - Psoas Muscle Release Tool for Hip Hook, Flexor, Back, Glute, Iliacus, and Neck Pain Trigger Point and Myofascial Release Tool - Night Black [Patent Pending]](https://m.media-amazon.com/images/I/61tN6K63x1L._AC_UL320_.jpg)

![]()
Psoas muscle and nerve-sheath sarcoma
The psoas muscle is located in the iliopsoas compartment of the body. Psoas muscle sarcoma is an uncommon condition that can cause malignant psoas syndrome (MPS), a rare clinical syndrome that significantly impacts the quality of life of terminally ill patients through metastatic infiltration of the psoas major muscle. This infiltration results in neurological symptoms such as painful fixed flexion of the ipsilateral hip, weakness in the leg and back, and proximal lumbosacral plexopathy.
MPS was first described by Stevens and Gonet in 1990 and has been identified in advanced-stage cancer patients. The diagnosis of MPS can be confirmed through clinical evidence of proximal lumbosacral plexopathy, fixed flexion of the hip, associated limitation of movement, and imaging that demonstrates invasion of the iliopsoas muscle. The current literature on MPS is limited to case reports and outdated literature reviews, highlighting a need for more standardized, evidence-based management protocols.
Treatment of MPS is challenging, and cases often require aggressive strategies such as increased opioid dosage, epidural administration of opioids, nerve blocks, cordotomy, botulinum toxin injection, and radiation therapy. However, even with these interventions, some patients may not experience pain relief. Radiotherapy has been suggested as a potential management strategy for MPS, as it has shown favourable outcomes in some cases.
In one case, a 68-year-old woman with a sarcoma in the left psoas muscle at the L4 level presented with MPS symptoms. She underwent presurgical radiotherapy, resulting in significant pain control improvement without increasing analgesic medications. Following this, she underwent an L4 vertebrectomy, and the left psoas muscle was resected from L3 to L5, sacrificing several nerves. The histopathology report indicated a low-grade but locally aggressive sarcoma, and the specimen was sent for expert opinion, confirming the diagnosis of a solitary fibrous tumour.
In summary, psoas muscle sarcoma is a rare condition that can lead to MPS, a clinically significant syndrome in terminally ill patients. The diagnosis and management of MPS are challenging due to limited literature and standardized protocols. Radiotherapy has shown promising results in treating psoas muscle sarcoma and improving MPS symptoms, as evident in the case study presented.
Muscle and Venules: What's the Connection?
You may want to see also
Explore related products






![]()
Schwannoma in the psoas muscle
Schwannomas are benign peripheral nerve sheath tumours, and their intramuscular localisation is exceptional. Schwannomas can occur wherever peripheral nerve Schwann cells are found. However, retroperitoneal schwannoma is extremely rare, with only about 15-16 cases reported in international literature.
The retroperitoneal approach provides direct access to the lumbar paraspinal lesion. To access the retroperitoneum and locate the ureter, right renal vein and kidney, and inferior vena cava, a Cattell manoeuvre can be performed.
In one case, a 51-year-old male presented with chronic lower back pain and paresthesia in the lower left region. An MRI revealed a neoplastic lesion about 6 cm in diameter in the left psoas major muscle, and the tumour was removed using Wiltse's approach. In another case, a 56-year-old male with a schwannoma in the right psoas muscle underwent a similar procedure.
The Heart's Nature: Exploring its Involuntary Muscle Mystery
You may want to see also
Explore related products

$9.99




![]()
Retroperitoneal surgery and the psoas muscle
The psoas muscle is retroperitoneal. Retroperitoneal surgery involving the psoas muscle is a rare but effective procedure for treating tumours in the retroperitoneal region. The retroperitoneal approach provides direct access to lumbar paraspinal lesions.
Retroperitoneal tumours are rare, constituting only 10-20% of all sarcomas, with an incidence of 0.3-0.4% per 100,000 population. They are challenging to evaluate and treat due to their rarity and frequent presentation in advanced stages in anatomically complex locations. However, surgical resection remains the optimal treatment for retroperitoneal tumours.
In one case, a 56-year-old male with a schwannoma in the right psoas muscle underwent successful tumour extirpation using the retroperitoneal approach. The procedure provided direct access to the lumbar paraspinal lesion. In another case, a patient with a large retroperitoneal tumour infiltrating the psoas major muscle underwent surgical resection, and at the six-month follow-up, the patient was asymptomatic.
Additionally, the psoas muscle retraction technique has been used in lumbar spine surgery to avoid injury to the lumbar plexus. This technique involves retracting the psoas muscle to gain lateral access to the lumbar spine, reducing the risk of complications associated with the traditional minimally invasive transpsoas approach.
Retroperitoneal surgery involving the psoas muscle resection has also been performed in patients with extensive retroperitoneal cancer. The procedure includes the resection of the femoral nerve, genitofemoral nerve, and ilioinguinal nerve, resulting in minimal morbidity and improved excision quality.
Pelvic Floor Muscles: What's the Deal with Involuntary Action?
You may want to see also
Frequently asked questions
The psoas muscle is bordered by great muscles like the diaphragm, the abdominal wall, and paraspinous muscles.
The psoas muscle is resected as part of a radical tumour excision in patients with extensive retroperitoneal cancer.
Surgery is the key treatment for retroperitoneal sarcoma (RPS) as the completeness of resection is the most important prognostic factor related to treatment.