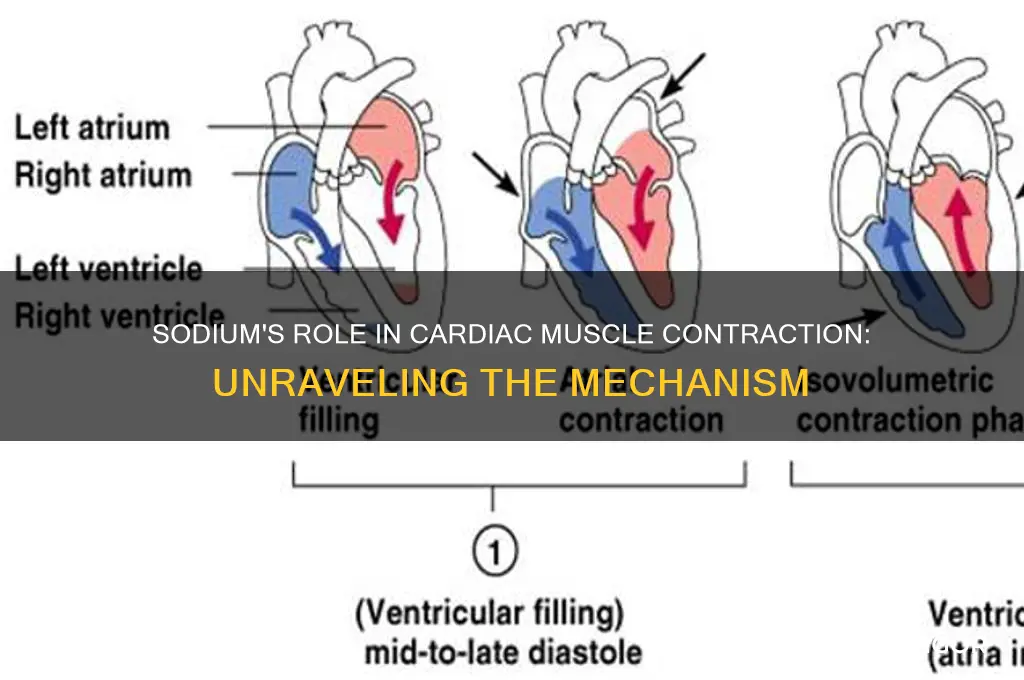
Cardiac muscle contraction is a complex process primarily driven by the movement of ions, particularly sodium, across cell membranes. Sodium plays a crucial role in initiating the electrical impulse that triggers contraction. When a cardiac muscle cell is at rest, sodium ions are concentrated outside the cell, creating a voltage difference known as the resting membrane potential. Upon stimulation, sodium channels open, allowing a rapid influx of sodium ions into the cell, which depolarizes the membrane and generates an action potential. This electrical signal propagates through the heart, leading to the release of calcium ions from intracellular stores, which ultimately bind to troponin and enable the interaction between actin and myosin filaments, resulting in muscle contraction. Thus, sodium is essential for the initial phase of the cardiac contraction cycle, setting off the cascade of events that ensure the heart’s rhythmic pumping action.
| Characteristics | Values |
|---|---|
| Ion Involved | Sodium (Na⁺) |
| Primary Role | Initiates the action potential in cardiac muscle cells |
| Mechanism | Sodium influx through voltage-gated sodium channels (Nav1.5) during phase 0 of the action potential |
| Duration | Rapid and transient (lasting ~1-2 ms) |
| Threshold Potential | Approximately -70 mV |
| Resulting Depolarization | Rapid rise in membrane potential to +30 mV |
| Subsequent Event | Activation of voltage-gated calcium channels (ICa,L) and calcium influx |
| Calcium's Role | Triggers calcium-induced calcium release from the sarcoplasmic reticulum, leading to muscle contraction |
| Repolarization | Sodium channels inactivate quickly, allowing potassium efflux to restore resting potential |
| Clinical Significance | Sodium channel dysfunction can lead to arrhythmias (e.g., Long QT syndrome, Brugada syndrome) |
| Pharmacological Target | Sodium channel blockers (e.g., Class I antiarrhythmic drugs) are used to manage arrhythmias |
Explore related products






What You'll Learn
![]()
Sodium-Potassium Pump Role
The sodium-potassium pump, also known as the Na⁺/K⁺ ATPase, plays a pivotal role in cardiac muscle contraction by maintaining the electrochemical gradients of sodium (Na⁺) and potassium (K⁺) ions across the cell membrane. This pump is an integral membrane protein that actively transports 3 Na⁺ ions out of the cell and 2 K⁺ ions into the cell for every ATP molecule hydrolyzed. In cardiac muscle cells (cardiomyocytes), this process is essential for establishing the resting membrane potential, which is a critical prerequisite for the initiation of electrical impulses that lead to muscle contraction. Without the sodium-potassium pump, the cell would lose its ability to maintain this gradient, disrupting the electrical signaling necessary for contraction.
The role of the sodium-potassium pump is directly tied to the excitation-contraction coupling process in cardiac muscle. When an electrical impulse (action potential) reaches the cardiomyocyte, voltage-gated sodium channels open, allowing a rapid influx of Na⁺ ions. This influx depolarizes the cell membrane, triggering the opening of voltage-gated calcium (Ca²⁺) channels. The sodium-potassium pump ensures that the intracellular Na⁺ concentration remains low, allowing for a significant driving force for Na⁺ entry during depolarization. This rapid and transient influx of Na⁺ is crucial for propagating the action potential along the cell membrane, which ultimately leads to the release of Ca²⁺ from the sarcoplasmic reticulum and subsequent muscle contraction.
Moreover, the sodium-potassium pump indirectly supports the function of the sodium-calcium exchanger (NCX), another critical protein in cardiac muscle. The NCX uses the Na⁺ gradient established by the sodium-potassium pump to remove Ca²⁺ from the cytoplasm in exchange for Na⁺ entry. This mechanism is vital for lowering intracellular Ca²⁺ levels after contraction, allowing the muscle to relax. Without the sodium-potassium pump, the Na⁺ gradient would collapse, impairing the NCX's ability to regulate Ca²⁺, which would disrupt both contraction and relaxation phases of the cardiac cycle.
Additionally, the sodium-potassium pump contributes to the overall metabolic efficiency of cardiomyocytes. By maintaining low intracellular Na⁺ levels, it reduces the workload on other ion transport systems, conserving energy for other cellular processes. This is particularly important in cardiac muscle, which has high-energy demands due to its continuous contractile activity. Dysfunction of the sodium-potassium pump, often observed in heart failure or ischemia, leads to Na⁺ overload, Ca²⁺ dysregulation, and impaired contractility, highlighting its central role in cardiac function.
In summary, the sodium-potassium pump is indispensable for cardiac muscle contraction by maintaining the Na⁺ and K⁺ gradients that drive electrical excitability and Ca²⁺ handling. Its role in establishing the resting membrane potential, supporting the action potential, and enabling Ca²⁺ regulation via the NCX underscores its importance in the excitation-contraction coupling process. Any compromise in its function can lead to severe cardiac dysfunction, emphasizing its critical role in maintaining heart health.
Buspar and Muscle Cramps: What's the Link?
You may want to see also
Explore related products






![]()
Action Potential Generation
The process of action potential generation in cardiac muscle is a complex yet fascinating mechanism that underlies the heart's ability to contract rhythmically. It begins with the movement of ions, particularly sodium, across the cell membrane. In cardiac muscle cells, also known as cardiomyocytes, the resting membrane potential is approximately -90 mV, which means the inside of the cell is negatively charged compared to the outside. This polarization is primarily due to the distribution of ions, with a higher concentration of sodium ions (Na+) outside the cell and a higher concentration of potassium ions (K+) inside.
When a stimulus is strong enough to initiate an action potential, it triggers the opening of voltage-gated sodium channels in the cell membrane. These channels are highly selective and allow only sodium ions to pass through. As the sodium channels open, there is a rapid influx of Na+ ions into the cell, driven by the electrochemical gradient. This sudden rush of positively charged sodium ions depolarizes the cell membrane, causing the membrane potential to rapidly rise towards zero and then slightly beyond, typically reaching around +30 mV. This phase is known as the depolarization phase and is critical for the initiation of cardiac muscle contraction.
Following depolarization, the sodium channels quickly inactivate, halting the influx of Na+ ions. Simultaneously, voltage-gated potassium channels open, allowing K+ ions to flow out of the cell. This efflux of positively charged potassium ions repolarizes the cell membrane, returning the membrane potential back toward the resting state. The repolarization phase is essential to reset the cell for the next action potential. During this phase, the membrane potential overshoots the resting potential slightly, creating a brief period of hyperpolarization before stabilizing back at the resting membrane potential.
The role of sodium in action potential generation is pivotal, as it provides the initial depolarizing current that triggers the entire sequence of events. However, sodium alone does not sustain the action potential; the coordinated activity of other ions, particularly potassium and calcium, is also crucial. In cardiac muscle, calcium ions (Ca2+) play a significant role in both the electrical signaling and the mechanical contraction process. Calcium influx occurs during the plateau phase of the action potential, which is unique to cardiac and skeletal muscle cells, and is mediated by voltage-gated calcium channels.
The interplay between sodium, potassium, and calcium ions ensures that the action potential in cardiac muscle is prolonged compared to that in neurons, allowing for a more sustained contraction necessary for effective pumping of blood. This prolonged action potential is also why cardiac muscle cells are described as having an automaticity—the ability to generate their own electrical impulses without external stimulation. This property is vital for the heart's pacemaker cells, which initiate each heartbeat. Understanding the role of sodium and other ions in action potential generation provides valuable insights into the mechanisms of cardiac function and highlights the importance of ion channel regulation in maintaining cardiovascular health.
Precocet and Muscle Tightness: What's the Link?
You may want to see also
Explore related products






![]()
Sodium Channel Function
The contraction of cardiac muscle, essential for the heart's pumping function, is intricately tied to the role of sodium channels in cardiomyocytes. Sodium channels are integral membrane proteins that facilitate the rapid influx of sodium ions (Na⁺) into the cell. This process is a critical first step in the cardiac action potential, which ultimately leads to muscle contraction. The primary function of sodium channels in this context is to initiate depolarization, the phase where the cell's membrane potential rapidly shifts from negative to positive. This depolarization is a prerequisite for the subsequent opening of calcium channels, which are responsible for the calcium influx necessary for contraction.
Sodium channels in cardiac muscle are voltage-gated, meaning they open and close in response to changes in the membrane potential. At rest, the cell membrane is polarized, and sodium channels are closed. When a stimulus causes a slight depolarization, these channels open, allowing a rapid influx of Na⁺ ions. This influx further depolarizes the membrane, creating a positive feedback loop that ensures the action potential reaches a threshold. The rapid and transient nature of sodium influx is due to the channels' inherent properties: they activate quickly but also inactivate rapidly, closing within milliseconds to prevent excessive sodium entry.
The specific sodium channels involved in cardiac muscle are primarily the Nav1.5 subtype, encoded by the *SCN5A* gene. These channels are highly specialized for the heart's unique electrical needs, ensuring that the action potential propagates efficiently throughout the myocardium. Mutations in *SCN5A* can lead to disorders such as long QT syndrome or Brugada syndrome, highlighting the critical role of sodium channels in maintaining normal cardiac function. The precise timing and amplitude of sodium influx are vital for synchronizing contraction across the heart, ensuring that the atria and ventricles work in harmony.
Another key aspect of sodium channel function is their role in maintaining the resting membrane potential. While potassium channels are primarily responsible for keeping the cell hyperpolarized at rest, sodium channels contribute by remaining closed until activated. This balance between sodium and potassium gradients is essential for creating the electrochemical environment necessary for action potential generation. Without functional sodium channels, the initial depolarization phase would be absent, preventing the downstream events that lead to calcium release and muscle contraction.
In summary, sodium channel function in cardiac muscle is pivotal for initiating the electrical signal that drives contraction. By mediating the rapid influx of Na⁺ ions, these channels trigger depolarization, setting off a chain of events that culminate in calcium-induced muscle contraction. Their voltage-gated nature, rapid kinetics, and specificity to cardiac tissue make them indispensable for heart function. Understanding their role not only sheds light on normal physiology but also provides insights into pathologies arising from their dysfunction.
Low C-Peptide: The Link to Muscle Cramps
You may want to see also
Explore related products





![]()
Calcium Release Mechanism
The contraction of cardiac muscle is a complex process that relies heavily on the precise regulation of calcium ions (Ca²⁺). While sodium (Na⁺) plays a crucial role in initiating the electrical impulse that triggers contraction, the actual mechanism of muscle fiber shortening is driven by calcium. The calcium release mechanism is a pivotal step in this process, ensuring that calcium ions are released from intracellular stores to activate the contractile machinery.
At the core of the calcium release mechanism is the sarcoplasmic reticulum (SR), a specialized network of tubules within cardiac muscle cells. The SR acts as a reservoir for calcium ions, storing them at high concentrations. When an electrical signal, known as an action potential, reaches the muscle cell, it triggers the opening of voltage-gated L-type calcium channels in the cell membrane. A small influx of calcium ions through these channels serves as a signal to activate ryanodine receptors (RyR2) located on the SR membrane. This activation is a critical step in the calcium release mechanism, as it initiates the release of a larger amount of calcium ions from the SR into the cytoplasm.
The process by which RyR2 receptors open in response to the initial calcium influx is known as calcium-induced calcium release (CICR). This mechanism amplifies the calcium signal, ensuring that a sufficient concentration of calcium ions is available to bind to troponin, a protein complex on the thin (actin) filaments of the muscle fiber. When calcium binds to troponin, it causes a conformational change that exposes binding sites for myosin heads on the thick (myosin) filaments. This interaction between actin and myosin is the fundamental event that leads to muscle contraction.
Following contraction, the calcium release mechanism must be tightly regulated to allow muscle relaxation. This is achieved through the active reuptake of calcium ions into the SR by sarcoplasmic reticulum Ca²⁺ ATPase (SERCA) pumps. These pumps use energy from ATP to transport calcium ions back into the SR, lowering cytoplasmic calcium levels. Additionally, some calcium ions are extruded from the cell via sodium-calcium exchangers in the cell membrane, further contributing to the restoration of resting calcium concentrations.
In summary, the calcium release mechanism is a highly coordinated process that involves the synchronized activity of L-type calcium channels, RyR2 receptors, and SERCA pumps. This mechanism ensures that calcium ions are released in a timely and controlled manner to initiate contraction and subsequently removed to allow relaxation. While sodium plays a role in triggering the initial electrical signal, it is the calcium release mechanism that directly drives the contraction of cardiac muscle fibers. Understanding this mechanism is essential for comprehending the physiology of cardiac muscle and the pathophysiology of conditions where calcium handling is impaired.
Cramping and Straining: Are They Related?
You may want to see also
Explore related products

$8.1 $13.99





![]()
Excitation-Contraction Coupling Process
The excitation-contraction coupling process in cardiac muscle is a complex and highly coordinated sequence of events that translates an electrical signal into mechanical contraction. This process is essential for the heart's ability to pump blood effectively and is intricately linked to the role of sodium ions (Na⁺) in initiating the sequence. It begins with the generation of an action potential in the cardiac muscle cells, known as cardiomyocytes. When the heart is stimulated, sodium channels in the cell membrane open, allowing a rapid influx of Na⁺ ions. This influx depolarizes the cell membrane, creating the rising phase of the action potential. The sodium-driven depolarization is critical because it triggers the subsequent steps that lead to muscle contraction.
Following the sodium influx, the depolarization of the cell membrane activates voltage-gated L-type calcium (Ca²⁺) channels in the sarcolemma (the cell membrane of muscle cells). These channels allow a small amount of Ca²⁺ to enter the cell, which acts as a secondary messenger. This initial Ca²⁺ entry is not sufficient to cause contraction on its own but instead binds to ryanodine receptors (RyR2) on the sarcoplasmic reticulum (SR), the cell's internal calcium store. The binding of Ca²⁺ to RyR2 triggers the opening of these receptors, leading to a rapid release of Ca²⁺ from the SR into the cytoplasm. This process, known as calcium-induced calcium release (CICR), results in a significant increase in cytoplasmic Ca²⁺ concentration, which is the key event that initiates muscle contraction.
The released Ca²⁺ ions bind to troponin, a protein complex located on the thin (actin) filaments of the sarcomere, the basic contractile unit of muscle. This binding causes a conformational change in the troponin-tropomyosin complex, exposing the myosin-binding sites on the actin filaments. Myosin heads can then attach to these sites, forming cross-bridges and pulling the actin filaments toward the center of the sarcomere. This sliding filament mechanism shortens the sarcomere length, leading to muscle contraction. The role of sodium in this phase is indirect but crucial, as it initiates the action potential that ultimately leads to the release of calcium, the primary mediator of contraction.
Termination of the contraction phase is equally important for the cardiac cycle and involves the removal of Ca²⁺ from the cytoplasm. As the action potential repolarizes, L-type calcium channels close, stopping the influx of external Ca²⁺. Simultaneously, the Ca²⁺-ATPase pump (SERCA) on the SR actively transports Ca²⁺ back into the SR, lowering cytoplasmic Ca²⁺ levels. Additionally, the sodium-calcium exchanger (NCX) in the sarcolemma removes one Ca²⁺ ion from the cell in exchange for three Na⁺ ions, further reducing cytoplasmic Ca²⁺. This decrease in Ca²⁺ concentration causes the troponin-tropomyosin complex to return to its inhibitory position, blocking myosin-binding sites and allowing the muscle to relax.
In summary, the excitation-contraction coupling process in cardiac muscle is a sodium-initiated, calcium-mediated mechanism. Sodium ions play a pivotal role by triggering the action potential, which leads to calcium release from the sarcoplasmic reticulum. Calcium, in turn, activates the contractile machinery, while its subsequent removal allows relaxation. This intricate interplay ensures the rhythmic and efficient contraction of the heart, highlighting the essential role of both sodium and calcium in cardiac function. Understanding this process is fundamental to comprehending how cardiac muscle contracts and how disruptions in this mechanism can lead to cardiac disorders.
Anesthesia Side Effects: Muscle Aches and Pains Explained
You may want to see also
Frequently asked questions
Sodium ions (Na⁺) initiate the electrical impulse (action potential) in cardiac muscle cells by rapidly flowing into the cell, causing depolarization, which triggers the contraction process.
Sodium enters cardiac muscle cells through voltage-gated sodium channels, which open in response to a stimulus, allowing Na⁺ to rush into the cell and start the action potential.
After sodium enters the cell, it is quickly pumped out by the sodium-potassium pump (Na⁺/K⁺ ATPase) to restore the cell's resting membrane potential, preparing it for the next contraction.
Yes, a severe lack of sodium (hyponatremia) can disrupt the electrical signaling in cardiac muscle cells, leading to irregular heart rhythms (arrhythmias) and impaired contraction.
Sodium's influx triggers the opening of calcium channels, allowing calcium ions (Ca²⁺) to enter the cell. Calcium then binds to troponin, initiating the sliding filament mechanism that causes muscle contraction.