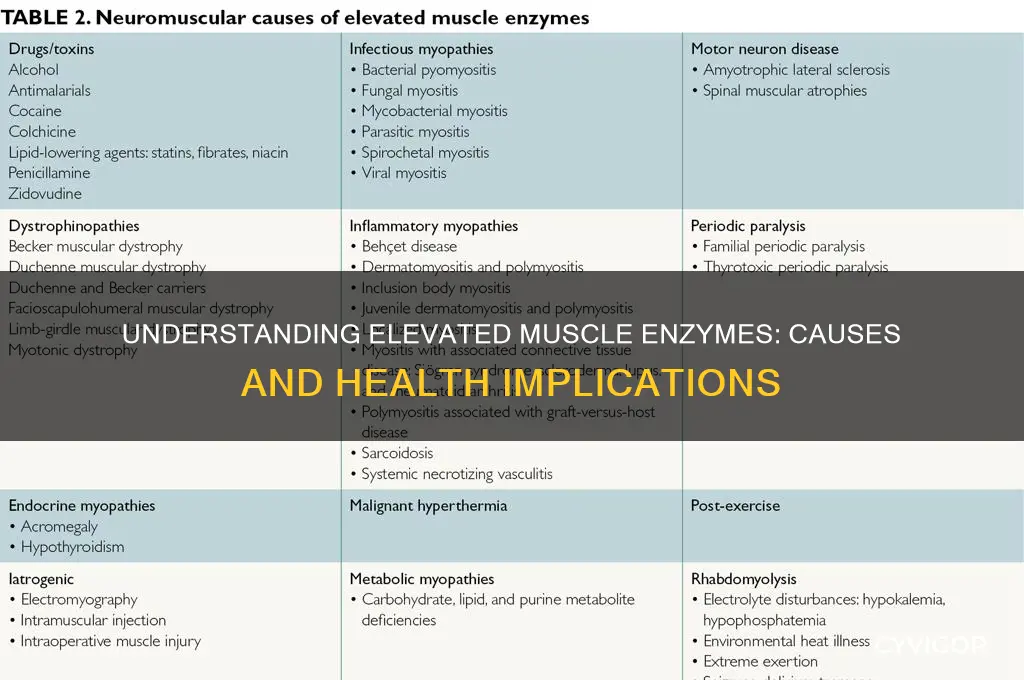
Elevated muscle enzymes, such as creatine kinase (CK), lactate dehydrogenase (LDH), and aldolase, often indicate muscle damage or injury. Common causes include strenuous physical activity, trauma, or conditions like rhabdomyolysis, where muscle tissue breaks down rapidly. Certain medications, autoimmune disorders (e.g., polymyositis), and genetic diseases (e.g., muscular dystrophy) can also lead to elevated levels. Additionally, infections, electrolyte imbalances, and metabolic disorders may contribute to this elevation. Understanding the underlying cause is crucial for appropriate diagnosis and treatment to prevent complications like kidney damage or chronic muscle dysfunction.
Explore related products

![Prime Screen [5 Pack] 6 Panel Urine Drug Test Kit (THC-Marijuana, BZO-Benzos, MET-Meth, OPI, AMP, COC), WDOA-264](https://m.media-amazon.com/images/I/71hU5zzuEaL._AC_UL320_.jpg)
![Enzymedica, Repair Gold, Proteolytic Enzymes, Joint Support Supplement,[a] Promotes Muscle Recovery & Tissue Function, 30 Count](https://m.media-amazon.com/images/I/61CaZtmfjaL._AC_UL320_.jpg)

![[5 Pack] EZCHECK® 6-Panel Drug Test - at-Home Rapid Urine Screening Kit for 6 Most Used Drugs: (THC-Marijuana, BZO-Benzos, MET-Meth, OPI/MOP-Opiates, AMP-Amphetamine, COC)](https://m.media-amazon.com/images/I/71c1jjFYkLL._AC_UL320_.jpg)

What You'll Learn
- Intense Exercise: Strenuous physical activity can temporarily increase muscle enzyme levels due to muscle breakdown
- Muscle Injury: Trauma or damage to muscles releases enzymes like CK and aldolase into the bloodstream
- Inflammatory Myopathies: Conditions like polymyositis cause muscle inflammation, elevating enzymes such as CK and AST
- Medications: Statins, fibrates, and certain drugs can induce muscle damage, leading to elevated enzyme levels
- Genetic Disorders: Muscular dystrophies and metabolic myopathies often result in chronically elevated muscle enzymes
![]()
Intense Exercise: Strenuous physical activity can temporarily increase muscle enzyme levels due to muscle breakdown
Intense exercise, particularly strenuous physical activity that pushes the muscles beyond their usual capacity, can lead to a temporary elevation in muscle enzyme levels. This phenomenon is primarily attributed to muscle breakdown, a natural consequence of the mechanical stress and metabolic demands placed on the muscles during vigorous exercise. When muscles are subjected to intense contractions, especially in activities like weightlifting, high-intensity interval training (HIIT), or long-distance running, the muscle fibers can experience microscopic damage. This damage triggers the release of intracellular enzymes, such as creatine kinase (CK), lactate dehydrogenase (LDH), and aldolase, into the bloodstream. These enzymes are normally contained within muscle cells but are released when the cell membranes are compromised due to excessive strain.
The release of muscle enzymes during intense exercise is a direct result of the physiological stress placed on the muscles. During strenuous activity, the muscles require more oxygen and energy than the body can readily supply, leading to the accumulation of metabolic byproducts like lactic acid. This metabolic stress, combined with mechanical tension, causes muscle fibers to stretch and sometimes tear. As the muscle cells repair themselves post-exercise, enzymes leak into the bloodstream, causing their levels to rise temporarily. This elevation is often more pronounced in individuals who are unaccustomed to such intense activity or those who engage in eccentric exercises, which involve muscle lengthening under tension, such as downhill running or lowering weights.
It is important to note that the elevation of muscle enzymes due to intense exercise is generally transient and not a cause for concern in healthy individuals. The body is well-equipped to handle this type of muscle damage, and the enzymes typically return to normal levels within 24 to 72 hours after exercise, depending on the intensity and duration of the activity. However, monitoring enzyme levels can be useful in assessing the extent of muscle damage, particularly in athletes or individuals undergoing rigorous training programs. Elevated enzyme levels may indicate the need for adequate recovery time to prevent overuse injuries or more severe muscle damage.
To mitigate the temporary increase in muscle enzymes caused by intense exercise, proper hydration, nutrition, and recovery strategies are essential. Consuming adequate protein and carbohydrates before and after exercise can support muscle repair and reduce the extent of muscle breakdown. Additionally, incorporating rest days and progressive training techniques can help the muscles adapt to higher levels of stress over time, minimizing enzyme release. For those new to intense physical activity, gradually increasing the intensity and duration of workouts can also reduce the risk of excessive muscle damage and enzyme elevation.
In summary, intense exercise can temporarily elevate muscle enzyme levels due to the breakdown of muscle fibers caused by mechanical and metabolic stress. This elevation is a normal physiological response to strenuous activity and is typically resolved with proper recovery. Understanding this process allows individuals to approach intense exercise with informed strategies to support muscle health and optimize performance while minimizing the risk of injury.
Yogurt Allergy and Muscle Pain: Is There a Link?
You may want to see also
Explore related products






![]()
Muscle Injury: Trauma or damage to muscles releases enzymes like CK and aldolase into the bloodstream
Muscle injuries, whether acute or chronic, are a significant cause of elevated muscle enzymes in the bloodstream. When muscles undergo trauma or damage, the integrity of muscle fibers is compromised, leading to the release of intracellular contents into the surrounding tissues and circulation. Among these contents are enzymes such as creatine kinase (CK) and aldolase, which are normally confined within muscle cells. CK, in particular, is highly concentrated in skeletal and cardiac muscles, making it a sensitive marker for muscle injury. When muscle fibers are damaged due to direct trauma, overexertion, or repetitive strain, the cell membranes rupture, allowing CK and aldolase to leak into the bloodstream. This elevation in enzyme levels is often detected in blood tests and serves as a diagnostic indicator of muscle injury.
The mechanism of enzyme release is directly tied to the extent and type of muscle damage. Acute injuries, such as those caused by a direct blow, fall, or sudden strenuous activity, result in immediate and significant increases in CK and aldolase levels. For example, athletes who experience muscle strains or contusions often show marked elevations in these enzymes within hours of the injury. Chronic muscle damage, on the other hand, may result from prolonged overuse, inflammatory conditions like polymyositis, or metabolic disorders such as muscular dystrophy. In these cases, enzyme levels may rise gradually and persist over time, reflecting ongoing muscle breakdown. Understanding the context of the injury—whether acute or chronic—is crucial for interpreting elevated enzyme levels accurately.
Elevated CK and aldolase levels are not only markers of muscle injury but also provide insights into the severity of the damage. Mild injuries typically cause modest increases in enzyme levels, while severe injuries, such as rhabdomyolysis (a condition where muscle tissue breaks down rapidly), lead to dramatic elevations. In rhabdomyolysis, the massive release of CK and other muscle constituents can overwhelm the kidneys, leading to acute kidney injury. Monitoring these enzymes is therefore essential not only for diagnosing muscle injury but also for assessing the risk of complications. Clinicians often correlate enzyme levels with symptoms, physical examination findings, and imaging studies to determine the appropriate management strategy.
It is important to note that while CK and aldolase are primarily associated with muscle injury, they are not specific to it. Other conditions, such as myocardial infarction (elevated CK-MB isoform) or liver disease, can also cause enzyme elevations. However, in the context of muscle trauma or damage, the pattern and degree of elevation often point clearly to a musculoskeletal origin. Patients with elevated muscle enzymes should undergo a thorough history and physical examination to identify potential causes, such as recent physical activity, medication use (e.g., statins), or underlying systemic disorders. This comprehensive approach ensures accurate diagnosis and targeted treatment.
In summary, muscle injury due to trauma or damage is a common cause of elevated CK and aldolase levels in the bloodstream. The release of these enzymes occurs when muscle fibers are disrupted, allowing intracellular contents to escape into circulation. The degree and duration of elevation depend on the type and severity of the injury, with acute trauma causing rapid increases and chronic conditions leading to persistent elevations. Recognizing this relationship is vital for diagnosing muscle injuries, assessing their severity, and preventing complications. By focusing on the mechanisms of enzyme release and their clinical implications, healthcare providers can effectively manage patients with elevated muscle enzymes.
Understanding the Triggers of Rib Muscle Cramps
You may want to see also
Explore related products




![[1 Test Cup] 14-Panel EZCHECK® Multi-Drug Urine Test Cup – at-Home Instant Testing for 14 Substances - Fast Result in 5 mins - FSA/HSA Eligible](https://m.media-amazon.com/images/I/71Geu5JRvZL._AC_UL320_.jpg)

![]()
Inflammatory Myopathies: Conditions like polymyositis cause muscle inflammation, elevating enzymes such as CK and AST
Inflammatory myopathies are a group of rare autoimmune disorders characterized by chronic muscle inflammation, leading to muscle weakness and elevated levels of muscle enzymes in the blood. Among these conditions, polymyositis is one of the most well-known, primarily affecting skeletal muscles and causing significant morbidity. The inflammation associated with polymyositis results in the destruction of muscle fibers, releasing intracellular enzymes into the bloodstream. Two key enzymes, creatine kinase (CK) and aspartate aminotransferase (AST), are commonly elevated in these cases. CK is particularly specific to muscle damage, as it is present in high concentrations within muscle cells, while AST, though also found in other organs like the liver, is significantly elevated in muscle-related injuries.
The pathophysiology of polymyositis involves an autoimmune response where the body's immune system mistakenly attacks healthy muscle tissue. This immune-mediated damage triggers an inflammatory cascade, leading to the infiltration of immune cells into muscle fibers. As muscle cells are damaged or destroyed, their cellular contents, including CK and AST, leak into the circulation. Elevated CK levels are often the most sensitive indicator of muscle injury in inflammatory myopathies, with levels sometimes increasing to several times the upper limit of normal. AST levels also rise, though they may be less specific since they can be elevated in liver disease as well. Monitoring these enzyme levels is crucial for diagnosing and managing polymyositis, as they serve as biomarkers of disease activity and muscle damage.
Diagnosing inflammatory myopathies like polymyositis involves a multifaceted approach, including clinical evaluation, blood tests, electromyography, and muscle biopsies. Elevated CK and AST levels are often the initial red flags prompting further investigation. A muscle biopsy can confirm the presence of inflammation and immune cell infiltration, while blood tests may reveal autoantibodies associated with these conditions. Treatment focuses on suppressing the immune system to reduce inflammation and prevent further muscle damage. Corticosteroids are typically the first-line therapy, often combined with immunosuppressive agents for refractory cases. Physical therapy and rehabilitation are also essential to maintain muscle strength and function.
The prognosis for individuals with polymyositis varies, with early diagnosis and aggressive treatment improving outcomes. However, untreated or poorly managed cases can lead to progressive muscle weakness, disability, and complications such as dysphagia or respiratory muscle involvement. Regular monitoring of CK and AST levels helps assess treatment efficacy and disease progression. Patients with persistently elevated enzyme levels may require adjustments to their treatment regimen, emphasizing the importance of these enzymes as both diagnostic and prognostic markers in inflammatory myopathies.
In summary, inflammatory myopathies like polymyositis cause muscle inflammation through autoimmune mechanisms, leading to the destruction of muscle fibers and the release of intracellular enzymes such as CK and AST into the bloodstream. These elevated enzyme levels are critical for diagnosis, monitoring disease activity, and guiding treatment. Understanding the relationship between muscle inflammation and enzyme elevation is essential for effective management of these debilitating conditions, ensuring timely intervention and improved patient outcomes.
Unraveling Extreme Fatigue and Muscle Aches: Common Causes and Solutions
You may want to see also
Explore related products

![[5 Pack] Prime Screen 12 Panel Urine Test (AMP,BAR,BZO,COC,mAMP,MDMA,MOP/OPI 300,MTD,OXY,PCP,TCA,THC) - WDOA-7125](https://m.media-amazon.com/images/I/71Hy719lOfL._AC_UL320_.jpg)




![]()
Medications: Statins, fibrates, and certain drugs can induce muscle damage, leading to elevated enzyme levels
Medications, particularly statins and fibrates, are well-documented causes of elevated muscle enzyme levels due to their potential to induce myopathy or muscle damage. Statins, widely prescribed for lowering cholesterol, work by inhibiting HMG-CoA reductase, an enzyme critical for cholesterol synthesis in the liver. While effective, they can inadvertently affect muscle cells, which also rely on this pathway. This disruption can lead to muscle cell injury, releasing enzymes such as creatine kinase (CK) and transaminases into the bloodstream, resulting in elevated levels detectable through blood tests. Patients on statins may experience symptoms ranging from mild muscle pain to severe rhabdomyolysis, a life-threatening condition characterized by rapid muscle breakdown.
Fibrates, another class of lipid-lowering medications, can similarly contribute to muscle enzyme elevation. These drugs activate peroxisome proliferator-activated receptors (PPARs) to reduce triglycerides and increase HDL cholesterol. However, their mechanism can also interfere with muscle metabolism, causing inflammation and damage. When statins and fibrates are used in combination, the risk of myopathy is significantly heightened due to synergistic effects on muscle cells. Clinicians often monitor muscle enzyme levels in patients taking these medications to detect early signs of toxicity and prevent severe complications.
Certain other drugs, such as colchicine, antiviral agents (e.g., zidovudine), and antipsychotics, have also been associated with muscle damage and elevated enzyme levels. Colchicine, used to treat gout, can cause myotoxicity, particularly at high doses or in patients with renal impairment. Antiviral medications, especially those used in HIV/AIDS treatment, may lead to mitochondrial dysfunction in muscle cells, resulting in weakness and enzyme release. Antipsychotics, particularly older generations, can cause extrapyramidal symptoms or rhabdomyolysis in rare cases. Understanding the pharmacological profiles of these drugs is crucial for identifying and managing medication-induced myopathy.
The pathophysiology of drug-induced muscle damage often involves direct toxicity, metabolic disruption, or immune-mediated mechanisms. For instance, statins deplete Coenzyme Q10, an essential component of mitochondrial function, leading to energy depletion in muscle cells. Immune-mediated reactions, such as those seen with statins in some individuals, can also cause muscle inflammation and necrosis. Early recognition of symptoms like muscle pain, tenderness, or weakness, coupled with regular monitoring of CK levels, is essential for timely intervention. Discontinuing or adjusting the dosage of the offending medication is typically the first step in management.
Patients at higher risk for medication-induced muscle damage include those with renal or hepatic impairment, older adults, and individuals taking multiple medications that interact negatively. Genetic factors, such as variants in the SLCO1B1 gene, can also predispose individuals to statin-induced myopathy. Healthcare providers should carefully assess these risk factors before prescribing such medications and educate patients about potential symptoms. Alternative lipid-lowering strategies, such as lifestyle modifications or other drug classes, may be considered for patients who develop intolerance to statins or fibrates. Vigilance and proactive management are key to minimizing the risk of elevated muscle enzymes and associated complications from these medications.
Muscle Cramps and Convulsions: What's the Connection?
You may want to see also
Explore related products


![Prime Screen [5 Pack] 5 Panel Urine Drug Test Kit - Testing Instantly for 5 Different Drugs AMP, COC, MET (Meth), OPI, THC (Marijuana) - WDOA-254](https://m.media-amazon.com/images/I/71FsDMfvdFL._AC_UL320_.jpg)

![Prime Screen [5 Pack] 12 Panel Urine Drug Test Kit (AMP, BAR, BUP, Benzos BZO, COC, mAMP, MDMA, MOP, MTD, OXY, PCP, Marijuana THC) - WDOA-6125](https://m.media-amazon.com/images/I/51jbz+-PFBL._AC_UL320_.jpg)

![]()
Genetic Disorders: Muscular dystrophies and metabolic myopathies often result in chronically elevated muscle enzymes
Genetic disorders, particularly muscular dystrophies and metabolic myopathies, are significant causes of chronically elevated muscle enzymes. These conditions are inherited and involve mutations in genes responsible for muscle structure, function, or metabolism. Muscular dystrophies, such as Duchenne and Becker muscular dystrophy, result from mutations in the dystrophin gene, which is critical for maintaining muscle fiber integrity. Without functional dystrophin, muscle fibers become vulnerable to damage during contraction, leading to ongoing muscle breakdown. This chronic muscle damage releases enzymes like creatine kinase (CK), aldolase, and lactate dehydrogenase (LDH) into the bloodstream, causing persistently elevated levels.
Metabolic myopathies, on the other hand, are caused by defects in enzymes or transport proteins involved in energy production within muscle cells. Examples include glycogen storage diseases (e.g., McArdle disease) and fatty acid oxidation disorders. In these conditions, the inability to properly metabolize substrates like glycogen or fatty acids leads to energy depletion and muscle cell dysfunction. This metabolic stress triggers muscle fiber damage, releasing enzymes into the circulation. For instance, patients with McArdle disease often exhibit elevated CK levels due to recurrent muscle injury during exercise.
The chronic elevation of muscle enzymes in these genetic disorders serves as a key diagnostic marker. Elevated CK levels, in particular, are highly suggestive of muscular dystrophies or myopathies, prompting further genetic testing to identify the underlying mutation. However, the degree of enzyme elevation can vary widely among individuals, depending on the specific disorder, disease stage, and individual factors such as physical activity levels. Monitoring these enzymes over time also helps assess disease progression and response to therapy.
Management of these genetic disorders focuses on symptom relief, slowing disease progression, and preventing complications. For muscular dystrophies, treatments may include corticosteroids to improve muscle strength and function, while metabolic myopathies often require dietary modifications or supplementation to optimize energy metabolism. Physical therapy and assistive devices play a crucial role in maintaining mobility and quality of life. Despite these interventions, the chronic muscle damage inherent to these disorders ensures that enzyme levels remain elevated, reflecting ongoing muscle pathology.
In summary, genetic disorders like muscular dystrophies and metabolic myopathies lead to chronically elevated muscle enzymes due to persistent muscle damage or dysfunction. These conditions highlight the intricate relationship between genetic mutations, muscle metabolism, and enzyme release. Recognizing and understanding these patterns is essential for accurate diagnosis, management, and patient education in the context of inherited muscle diseases.
Muscle Spasms and Multiple Sclerosis: What's the Link?
You may want to see also
Frequently asked questions
Muscle enzymes, such as creatine kinase (CK), lactate dehydrogenase (LDH), and aldolase, are proteins found in muscle cells that play a crucial role in energy production and muscle function. Elevated levels of these enzymes in the blood can indicate muscle damage or disease.
Common causes include strenuous exercise, muscle injury or trauma, inflammatory muscle diseases (e.g., polymyositis), genetic disorders (e.g., muscular dystrophy), medications (e.g., statins), and metabolic conditions like hypothyroidism or electrolyte imbalances.
Yes, persistently elevated muscle enzymes may indicate serious conditions such as rhabdomyolysis (severe muscle breakdown), autoimmune disorders, or metabolic diseases. It’s important to consult a healthcare provider for proper evaluation and diagnosis.
Diagnosis involves blood tests to measure enzyme levels, along with medical history and physical exams. Treatment depends on the underlying cause, ranging from rest and hydration for exercise-induced elevation to medications or therapy for chronic conditions.






![Prime Screen 12 Panel Drug Test Kit - Instant Urine Testing Marijuana(THC),AMP,BAR,BZO,COC,mAMP,MDMA,MOP/OPI 300 Cut-Off Level,MTD,OXY,PCP,TCA -TDOA-7125 [5 Pack]](https://m.media-amazon.com/images/I/71oTnSSHRaL._AC_UL320_.jpg)
![Easy@Home Marijuana Urine Drug Test Kit [25 Pack] - THC Tests for Home Use, Weed Detox Testing Kits with 50 ng/ml Cutoff Level, #EDTH-114](https://m.media-amazon.com/images/I/716EWs27byL._AC_UL320_.jpg)


![[25 Pack] U-CATCH Plus Multi-Drug Test Kit for All: 12 Panel Urine Test Cup Rapid Drug Test at Home for Marijuana(THC),AMP,BAR,BUP,BZO,COC,MDMA,MET,MOP,MTD,OXY,PCP](https://m.media-amazon.com/images/I/61R3c9ksLLL._AC_UL320_.jpg)


















