Malignant hyperthermia (MH) is a rare, life-threatening condition triggered by certain anesthetic agents, characterized by a rapid and uncontrolled increase in body temperature, muscle rigidity, and metabolic acidosis. Muscle rigidity in MH is primarily caused by a genetic mutation in the ryanodine receptor 1 (RYR1) gene, which regulates calcium release in skeletal muscle cells. During exposure to triggering agents like volatile anesthetics or succinylcholine, the mutated RYR1 receptor malfunctions, leading to excessive calcium release from the sarcoplasmic reticulum. This sustained calcium influx causes prolonged muscle contraction, resulting in rigidity. The increased metabolic demand from continuous muscle activity further exacerbates hyperthermia and metabolic disturbances, making prompt recognition and treatment essential to prevent severe complications or fatality.
| Characteristics | Values |
|---|---|
| Genetic Mutation | Malignant hyperthermia (MH) is primarily caused by mutations in genes encoding ryanodine receptor 1 (RYR1) and, less commonly, calcium voltage-gated channel subunit alpha1S (CACNA1S). These mutations lead to abnormal calcium release from the sarcoplasmic reticulum in skeletal muscle cells. |
| Triggering Agents | Muscle rigidity in MH is typically triggered by volatile anesthetic agents (e.g., halothane, sevoflurane, isoflurane) and succinylcholine, which exacerbate abnormal calcium release in susceptible individuals. |
| Calcium Dysregulation | Excessive calcium release from the sarcoplasmic reticulum leads to sustained muscle fiber contraction, resulting in muscle rigidity and increased metabolic demand. |
| Metabolic Consequences | The sustained muscle contraction causes rapid ATP depletion, leading to metabolic acidosis, hyperkalemia, and rhabdomyolysis, further contributing to muscle rigidity and systemic complications. |
| Hyperthermia | The increased metabolic activity generates excessive heat, leading to hyperthermia, which exacerbates muscle rigidity and other symptoms of MH. |
| Autosomal Dominant Inheritance | MH susceptibility is inherited in an autosomal dominant pattern, meaning a single mutated copy of the gene (RYR1 or CACNA1S) is sufficient to cause the condition. |
| Clinical Presentation | Muscle rigidity is a hallmark symptom of MH, often accompanied by tachycardia, tachypnea, acidosis, and elevated creatine kinase levels. |
| Treatment | Immediate administration of dantrolene sodium is the primary treatment, as it inhibits calcium release from the sarcoplasmic reticulum, reversing muscle rigidity and other MH symptoms. |
| Prevention | Avoiding triggering agents in susceptible individuals and genetic testing for at-risk families are key preventive measures. |
Explore related products






What You'll Learn
- Genetic Mutations: RyR1 gene mutations disrupt calcium release, causing muscle rigidity in malignant hyperthermia
- Calcium Dysregulation: Excessive calcium release from sarcoplasmic reticulum leads to sustained muscle contraction
- Triggering Agents: Volatile anesthetics and succinylcholine induce abnormal muscle responses in susceptible individuals
- Metabolic Overload: Increased metabolism and ATP depletion contribute to muscle stiffness and rigidity
- Inflammatory Response: Elevated cytokines and systemic inflammation exacerbate muscle rigidity during malignant hyperthermia
![]()
Genetic Mutations: RyR1 gene mutations disrupt calcium release, causing muscle rigidity in malignant hyperthermia
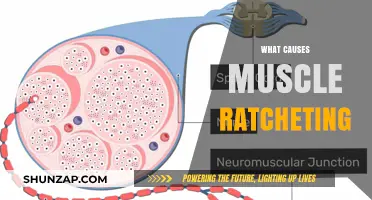
Malignant hyperthermia (MH) is a life-threatening condition characterized by rapid skeletal muscle rigidity, hyperthermia, and metabolic acidosis, typically triggered by certain anesthetic agents. At the core of this disorder are genetic mutations, specifically in the RyR1 gene, which encodes the ryanodine receptor 1 (RyR1) protein. This protein plays a critical role in calcium regulation within muscle cells. In individuals with MH, mutations in the RyR1 gene disrupt the normal function of the RyR1 receptor, leading to dysregulated calcium release and subsequent muscle rigidity. Understanding this genetic basis is essential for diagnosing, managing, and preventing MH.
The RyR1 receptor is a calcium release channel located on the sarcoplasmic reticulum (SR) of skeletal muscle cells. During normal muscle contraction, a small influx of calcium through the cell membrane triggers the RyR1 channel to open, releasing a larger amount of calcium from the SR into the cytoplasm. This calcium binds to troponin, initiating muscle contraction. In MH, mutations in the RyR1 gene cause the channel to become hypersensitive or leaky, leading to an abnormal release of calcium ions even in the absence of appropriate triggers. This excessive calcium release results in sustained muscle contraction, manifesting as rigidity.
RyR1 gene mutations are inherited in an autosomal dominant manner, meaning a single mutated copy of the gene is sufficient to cause MH. Over 700 mutations in the RyR1 gene have been identified, each with varying degrees of severity and penetrance. These mutations alter the structure or function of the RyR1 receptor, impairing its ability to regulate calcium release effectively. For example, some mutations cause the channel to remain partially open, while others disrupt its interaction with regulatory proteins like calstabin1, which normally stabilizes the closed state of the channel. This dysregulation of calcium homeostasis is the primary mechanism underlying muscle rigidity in MH.
The clinical implications of RyR1 mutations are profound, as they render individuals susceptible to MH episodes during exposure to triggering agents such as volatile anesthetics (e.g., halothane, sevoflurane) or the muscle relaxant succinylcholine. When these agents interact with the mutated RyR1 receptor, they further enhance calcium release, exacerbating muscle rigidity and leading to a cascade of metabolic and physiologic abnormalities. Early recognition of MH and prompt administration of the antidote, dantrolene sodium, which inhibits calcium release from the SR, are critical to preventing severe complications or fatalities.
In summary, RyR1 gene mutations are the primary genetic cause of muscle rigidity in malignant hyperthermia. By disrupting calcium release mechanisms in skeletal muscle cells, these mutations lead to uncontrolled muscle contraction and rigidity. Identifying individuals with RyR1 mutations through genetic testing is crucial for risk stratification and preventive management. Ongoing research into the specific mechanisms of RyR1 dysfunction continues to enhance our understanding of MH and may lead to novel therapeutic strategies in the future.
Muscle Soreness: Weight Gain or Loss?
You may want to see also
Explore related products






![]()
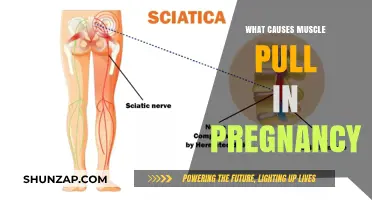
Calcium Dysregulation: Excessive calcium release from sarcoplasmic reticulum leads to sustained muscle contraction
Calcium dysregulation plays a central role in the pathophysiology of muscle rigidity in malignant hyperthermia (MH). At the core of this process is the excessive release of calcium ions from the sarcoplasmic reticulum (SR), a specialized structure within muscle cells that stores calcium. Under normal conditions, calcium release from the SR is tightly regulated, allowing for precise control of muscle contraction and relaxation. However, in individuals with MH, genetic mutations—most commonly in the *RYR1* gene encoding the ryanodine receptor (RyR1)—lead to abnormal functioning of this calcium release channel. During exposure to triggering agents like volatile anesthetics or succinylcholine, the mutated RyR1 becomes hyperresponsive, resulting in an uncontrolled and sustained release of calcium into the cytoplasm.
This excessive calcium release initiates a cascade of events that culminates in sustained muscle contraction. Calcium ions bind to troponin C on the actin filaments, exposing myosin-binding sites and enabling cross-bridge formation. Normally, calcium is rapidly re-sequestered into the SR by the sarco/endoplasmic reticulum calcium ATPase (SERCA) pump, allowing muscles to relax. In MH, the prolonged elevation of cytoplasmic calcium due to excessive release and impaired reuptake disrupts this cycle. The continuous interaction between actin and myosin filaments leads to rigid, unrelaxed muscles, a hallmark of MH. This sustained contraction not only contributes to muscle rigidity but also increases metabolic demand, leading to further complications such as hyperthermia and metabolic acidosis.
The role of the sarcoplasmic reticulum in calcium dysregulation cannot be overstated. In MH-susceptible individuals, the SR becomes a source of pathological calcium overload rather than a regulated storage compartment. The mutated RyR1 channel exhibits increased sensitivity to triggering agents, leading to a "leaky" channel that releases calcium even in the absence of normal physiological stimuli. This leakiness is exacerbated during anesthesia, as volatile agents like halothane directly activate the mutated RyR1, further amplifying calcium release. The resulting intracytoplasmic calcium overload overwhelms the SERCA pump's capacity to re-sequester calcium, perpetuating the cycle of sustained muscle contraction and rigidity.
Clinically, the muscle rigidity caused by calcium dysregulation is a critical early sign of MH. It typically begins in the masseter muscles (jaw rigidity) and progresses to involve larger muscle groups, leading to generalized rigidity and increased oxygen consumption. If unrecognized or untreated, this rigidity contributes to the life-threatening hypermetabolic state of MH. Immediate management focuses on discontinuing triggering agents and administering dantrolene sodium, which inhibits calcium release from the SR by directly acting on RyR1. This intervention helps restore calcium homeostasis, alleviating muscle rigidity and preventing further complications. Understanding the mechanism of calcium dysregulation in MH is essential for early diagnosis and effective treatment, emphasizing the importance of recognizing the role of the sarcoplasmic reticulum in this disorder.
Steroids and Muscle Health: Uncovering Potential Risks of Damage
You may want to see also
Explore related products






![]()
Triggering Agents: Volatile anesthetics and succinylcholine induce abnormal muscle responses in susceptible individuals
Muscle rigidity in malignant hyperthermia (MH) is primarily triggered by the administration of specific pharmacological agents, notably volatile anesthetics and the depolarizing muscle relaxant succinylcholine. These agents induce an abnormal muscle response in genetically susceptible individuals, leading to a cascade of events that result in muscle rigidity, hyperthermia, and other life-threatening symptoms. The mechanism involves the dysregulation of calcium homeostasis within skeletal muscle cells, which is central to the pathophysiology of MH.
Volatile anesthetics, such as halothane, sevoflurane, isoflurane, and desflurane, are potent triggers of MH in susceptible individuals. These agents interact with the ryanodine receptor type 1 (RYR1) on the sarcoplasmic reticulum of muscle cells. In normal individuals, RYR1 regulates the release of calcium ions into the cytoplasm, which is essential for muscle contraction. However, in individuals with mutations in the *RYR1* gene, volatile anesthetics cause an abnormal, sustained release of calcium, leading to prolonged muscle contraction and rigidity. This excessive calcium release also activates metabolic pathways that increase oxygen consumption and heat production, contributing to hyperthermia.
Succinylcholine, a depolarizing muscle relaxant, is another critical triggering agent in MH. It acts by binding to nicotinic acetylcholine receptors on the muscle cell membrane, causing prolonged depolarization. In susceptible individuals, this depolarization further exacerbates the abnormal calcium release from the sarcoplasmic reticulum via RYR1. The combined effect of succinylcholine and volatile anesthetics creates a synergistic response, dramatically increasing the risk of muscle rigidity and the onset of MH. This is why succinylcholine is considered particularly dangerous in individuals with MH susceptibility.
The abnormal muscle responses induced by these triggering agents are not limited to rigidity alone. They also lead to rapid ATP depletion due to sustained muscle contraction, which impairs cellular energy metabolism. This energy crisis, coupled with increased metabolic demand, results in the production of lactic acid and a subsequent metabolic acidosis. Additionally, the massive release of calcium and other intracellular contents into the bloodstream can cause systemic complications, including cardiac arrhythmias and renal failure.
In susceptible individuals, the use of triggering agents must be avoided to prevent MH. Alternative anesthetic techniques, such as total intravenous anesthesia (TIVA) using non-triggering agents like propofol and dexmedetomidine, are recommended. Rapid recognition and treatment of MH, including the administration of dantrolene sodium to inhibit calcium release from the sarcoplasmic reticulum, are crucial for managing this potentially fatal condition. Understanding the role of volatile anesthetics and succinylcholine in inducing abnormal muscle responses is essential for preventing and managing MH in clinical practice.
Bone Pain and Muscle Pain: What's the Link?
You may want to see also
Explore related products






![]()
Metabolic Overload: Increased metabolism and ATP depletion contribute to muscle stiffness and rigidity
Malignant hyperthermia (MH) is a life-threatening condition characterized by rapid skeletal muscle rigidity, hyperthermia, and metabolic acidosis, typically triggered by volatile anesthetics or succinylcholine. At the core of muscle rigidity in MH is metabolic overload, a phenomenon driven by dysregulated calcium homeostasis and excessive energy demands within muscle cells. In susceptible individuals, mutations in the *RYR1* gene encoding the ryanodine receptor (RYR1) lead to abnormal calcium release from the sarcoplasmic reticulum (SR) upon exposure to triggering agents. This prolonged calcium release activates ATP-dependent processes like muscle contraction and calcium reuptake, dramatically increasing metabolic demand.
The increased metabolic rate in MH rapidly depletes cellular ATP stores, as the energy required to maintain calcium cycling and muscle contraction exceeds the capacity of oxidative phosphorylation. ATP depletion compromises the function of critical ATP-dependent pumps, such as the sarco/endoplasmic reticulum Ca²⁺ ATPase (SERCA) and the plasma membrane Ca²⁺ ATPase (PMCA), which are essential for removing calcium from the cytoplasm and restoring muscle relaxation. Without sufficient ATP, calcium remains trapped in the cytoplasm, sustaining muscle contraction and leading to rigidity. This vicious cycle of ATP depletion and calcium overload is a hallmark of metabolic overload in MH.
Furthermore, the heightened metabolic activity in MH generates excessive heat, contributing to hyperthermia, which in turn accelerates ATP degradation and exacerbates metabolic overload. As ATP levels plummet, other ATP-dependent processes, such as the sodium-potassium pump, become impaired, leading to cellular swelling and further compromising muscle function. The cumulative effect of these processes results in sustained muscle stiffness and rigidity, which are clinically evident as rigidity, tachycardia, and elevated creatine kinase levels.
Addressing metabolic overload in MH requires immediate intervention to halt the cascade of events. Administration of dantrolene sodium, the mainstay treatment, inhibits calcium release from the SR, reducing metabolic demand and preserving ATP. Simultaneously, supportive measures such as cooling, hydration, and electrolyte management aim to mitigate the effects of hyperthermia and metabolic acidosis. Understanding the role of metabolic overload in MH underscores the importance of prompt recognition and treatment to prevent irreversible muscle damage and multiorgan failure.
In summary, metabolic overload in MH is a direct consequence of increased calcium-driven metabolic demands and ATP depletion, leading to muscle stiffness and rigidity. The interplay between dysregulated calcium homeostasis, ATP depletion, and hyperthermia creates a self-perpetuating cycle that requires urgent intervention. By targeting calcium release and supporting metabolic function, clinicians can effectively manage this critical condition and improve patient outcomes.
Inflammation and Lower Back Pain: What's the Link?
You may want to see also
Explore related products






![]()
Inflammatory Response: Elevated cytokines and systemic inflammation exacerbate muscle rigidity during malignant hyperthermia
Malignant hyperthermia (MH) is a life-threatening condition characterized by rapid skeletal muscle rigidity, hyperthermia, and metabolic acidosis, typically triggered by certain anesthetic agents. Among the multifaceted mechanisms contributing to muscle rigidity in MH, the inflammatory response plays a pivotal role. During MH, the abnormal release of calcium ions from the sarcoplasmic reticulum leads to sustained muscle contraction. This process is further exacerbated by the systemic inflammatory response, which is marked by the elevated release of pro-inflammatory cytokines such as interleukin-6 (IL-6), tumor necrosis factor-alpha (TNF-α), and interleukin-1β (IL-1β). These cytokines are released in response to cellular stress and tissue damage, creating a cascade of events that amplify muscle rigidity.
Elevated cytokine levels contribute to muscle rigidity by promoting systemic inflammation, which affects both muscle tissue and the broader physiological environment. Cytokines act on muscle fibers, increasing their excitability and sensitivity to calcium. This heightened sensitivity prolongs muscle contractions, making relaxation difficult. Additionally, cytokines induce the expression of adhesion molecules on endothelial cells, facilitating the infiltration of immune cells into muscle tissue. This immune cell infiltration further damages muscle fibers, releasing more intracellular contents and perpetuating the cycle of inflammation and rigidity. The interplay between cytokine release and muscle dysfunction creates a feed-forward loop that intensifies the rigidity observed in MH.
Systemic inflammation also impacts muscle rigidity by altering vascular function and oxygen delivery. Inflammatory mediators cause vasodilation and increased vascular permeability, leading to edema in muscle tissue. This edema compresses muscle fibers, impairing their ability to relax and contributing to rigidity. Furthermore, the inflammatory response diverts blood flow away from skeletal muscles, reducing oxygen and nutrient supply. Hypoxia and metabolic stress in muscle cells exacerbate calcium dysregulation, further sustaining contractions. The combination of vascular compromise and metabolic stress amplifies the rigidity and tissue damage characteristic of MH.
Another critical aspect of the inflammatory response in MH is its role in activating the coagulation cascade and promoting microthrombosis. Elevated cytokines, particularly IL-6 and TNF-α, stimulate the production of tissue factor by endothelial cells and monocytes, initiating coagulation. Microthrombi formation in muscle tissue impairs blood flow, leading to ischemia and further tissue damage. Ischemic muscle fibers release additional inflammatory mediators, creating a self-perpetuating cycle of inflammation, coagulation, and rigidity. This thromboinflammatory process significantly contributes to the severity and persistence of muscle rigidity during MH episodes.
In summary, the inflammatory response is a key driver of muscle rigidity in malignant hyperthermia, with elevated cytokines and systemic inflammation playing central roles. Cytokines enhance muscle excitability, promote immune cell infiltration, and induce vascular dysfunction, all of which exacerbate rigidity. The interplay between inflammation, coagulation, and metabolic stress creates a complex environment that sustains and worsens muscle contractions. Understanding these mechanisms underscores the importance of early intervention to mitigate inflammation and prevent the progression of MH. Targeting the inflammatory response may offer therapeutic opportunities to manage muscle rigidity and improve outcomes in MH patients.
Understanding Abdominal Muscle Cramps: Causes and Prevention Tips
You may want to see also
Frequently asked questions
Malignant hyperthermia is a life-threatening genetic disorder triggered by certain anesthetic agents, particularly volatile anesthetics and succinylcholine. It causes muscle rigidity due to uncontrolled calcium release from the sarcoplasmic reticulum in muscle cells, leading to sustained muscle contraction and stiffness.
In MH, mutations in the *RYR1* gene (encoding the ryanodine receptor) cause excessive calcium release from the sarcoplasmic reticulum in skeletal muscle cells. This elevated calcium triggers prolonged muscle contraction, resulting in rigidity and increased metabolic demand, which can lead to hyperthermia and metabolic acidosis.
Yes, muscle rigidity is often the earliest and most consistent sign of MH, sometimes appearing before hyperthermia develops. Rigidity can manifest as jaw stiffness, generalized muscle hardness, or increased end-tidal carbon dioxide levels, even if the body temperature has not yet risen significantly.