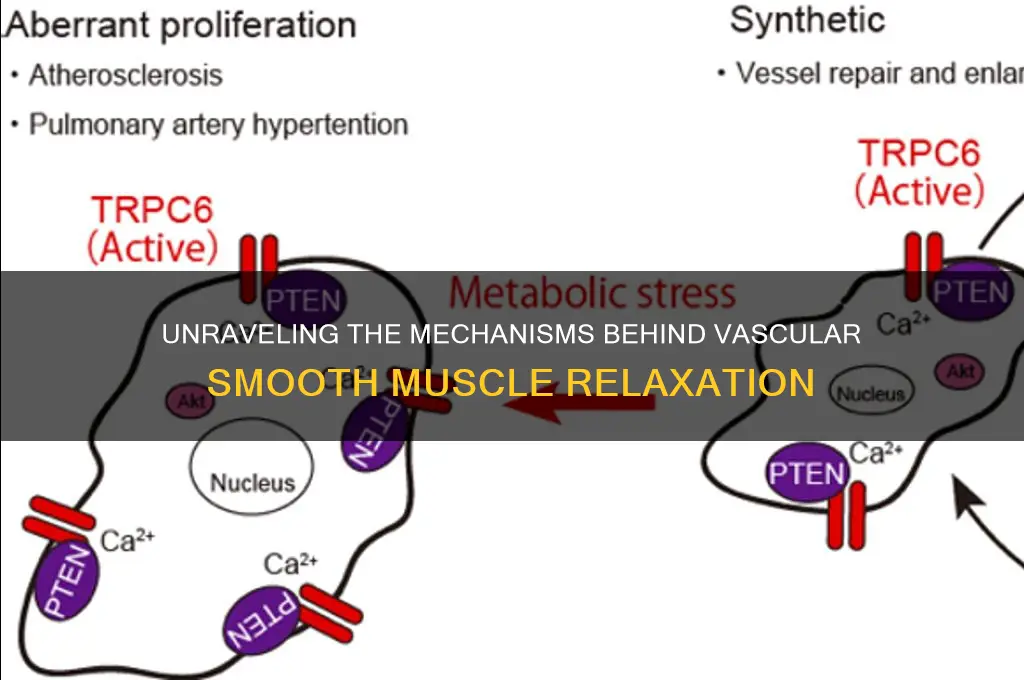
Vascular smooth muscle relaxation is a critical process in regulating blood flow and blood pressure, primarily mediated by the activation of specific signaling pathways and the release of vasodilatory substances. Key factors that induce relaxation include the activation of nitric oxide (NO) pathways, where NO produced by endothelial cells diffuses into smooth muscle cells, stimulating soluble guanylate cyclase to increase cyclic GMP levels, which in turn activates protein kinase G, leading to decreased calcium sensitivity and muscle relaxation. Additionally, prostacyclin (PGI2) and endothelial-derived hyperpolarizing factors (EDHFs) contribute by activating adenylate cyclase and hyperpolarizing the cell membrane, respectively. Other mechanisms involve the release of adenosine, bradykinin, and acetylcholine, which act on specific receptors to promote relaxation. Understanding these pathways is essential for developing therapies targeting hypertension and vascular diseases.
| Characteristics | Values |
|---|---|
| Nitric Oxide (NO) | Produced by endothelial cells, activates guanylate cyclase, increases cGMP, leading to relaxation. |
| Prostaglandins (PGI2) | Synthesized by endothelial cells, activates adenylate cyclase, increases cAMP, promotes relaxation. |
| Endothelium-Derived Hyperpolarizing Factor (EDHF) | Causes hyperpolarization of smooth muscle cells via potassium channels, leading to relaxation. |
| Adenosine | Activates A2 receptors, increases cAMP, promotes relaxation. |
| Potassium Channel Openers | Directly activate potassium channels, hyperpolarize smooth muscle cells, induce relaxation. |
| Calcium Channel Blockers | Inhibit calcium influx, reduce intracellular calcium, cause relaxation. |
| Beta-2 Adrenergic Agonists | Activate beta-2 receptors, increase cAMP, promote relaxation. |
| Nitrovasodilators (e.g., Nitroglycerin) | Release NO or NO-related compounds, increase cGMP, induce relaxation. |
| Hypercapnia (High CO2) | Increases intracellular H+ ions, activates potassium channels, promotes relaxation. |
| Acetylcholine (via M3 Receptors) | Activates M3 receptors on endothelial cells, releases NO, causes relaxation. |
| Atrial Natriuretic Peptide (ANP) | Activates guanylate cyclase, increases cGMP, promotes relaxation. |
| Bradykinin | Activates B2 receptors, releases NO and PGI2, causes relaxation. |
| Shear Stress | Mechanical force on endothelial cells, stimulates NO release, induces relaxation. |
| Hydrogen Sulfide (H2S) | Activates potassium channels, reduces intracellular calcium, promotes relaxation. |
| Carbon Monoxide (CO) | Activates soluble guanylate cyclase, increases cGMP, causes relaxation. |
| Magnesium | Competes with calcium, reduces intracellular calcium, promotes relaxation. |
Explore related products




What You'll Learn
- Nitric Oxide (NO) Signaling: NO activates soluble guanylate cyclase, increasing cGMP, reducing calcium, promoting relaxation
- Prostaglandins and EDHF: Vasodilatory prostaglandins and EDHF hyperpolarize membranes, decreasing calcium influx
- Adenosine Receptor Activation: Adenosine binds receptors, increases cAMP, reduces calcium, induces relaxation
- Acetylcholine and M3 Receptors: Acetylcholine activates M3 receptors, increases cAMP, promotes relaxation
- Calcium Channel Blockers: Block L-type calcium channels, reduce intracellular calcium, cause relaxation
![]()
Nitric Oxide (NO) Signaling: NO activates soluble guanylate cyclase, increasing cGMP, reducing calcium, promoting relaxation
Nitric oxide (NO) signaling plays a pivotal role in the relaxation of vascular smooth muscle, a process critical for regulating blood flow and vascular tone. When NO is released from endothelial cells or other sources, it diffuses rapidly to adjacent vascular smooth muscle cells. Upon entry, NO binds specifically to the heme moiety of soluble guanylate cyclase (sGC), a key enzyme in this signaling pathway. This binding event triggers a conformational change in sGC, activating its catalytic activity. The primary function of activated sGC is to catalyze the conversion of guanosine triphosphate (GTP) to cyclic guanosine monophosphate (cGMP), a critical second messenger in this pathway. The increase in cGMP levels initiates a cascade of events that ultimately lead to smooth muscle relaxation.
The elevation of cGMP activates cGMP-dependent protein kinases (PKG), which phosphorylate various target proteins involved in calcium regulation and contractility. One of the key targets of PKG is the phospholamban protein, which, when phosphorylated, increases the activity of the sarcoplasmic reticulum Ca²⁺-ATPase (SERCA). This enhances the uptake of calcium ions (Ca²⁺) from the cytosol into the sarcoplasmic reticulum, effectively reducing cytosolic calcium concentration. Additionally, PKG inhibits the activity of myosin light chain kinase (MLCK), a protein responsible for phosphorylating myosin light chains, which is essential for muscle contraction. By reducing MLCK activity, the phosphorylation of myosin light chains decreases, leading to a decrease in actin-myosin cross-bridge formation and subsequent muscle relaxation.
Another critical mechanism by which cGMP promotes relaxation involves the opening of potassium (K⁺) channels in the plasma membrane of smooth muscle cells. PKG phosphorylates and activates these channels, leading to an efflux of K⁺ ions. This efflux hyperpolarizes the cell membrane, making it less likely for voltage-gated calcium channels to open. As a result, calcium influx is reduced, further lowering cytosolic calcium levels. The combined effect of increased calcium sequestration by SERCA and decreased calcium entry through voltage-gated channels significantly reduces the availability of calcium for muscle contraction, promoting relaxation.
Furthermore, NO signaling indirectly modulates calcium sensitivity in vascular smooth muscle cells. PKG can phosphorylate and inhibit the activity of CPI-17, a protein that enhances the calcium sensitivity of MLCK. By reducing CPI-17 activity, the overall sensitivity of the contractile machinery to calcium is diminished, making it harder for the muscle to maintain a contracted state even in the presence of moderate calcium levels. This dual action of reducing calcium availability and decreasing calcium sensitivity ensures robust and sustained relaxation of vascular smooth muscle.
In summary, NO signaling initiates a well-coordinated series of events that culminate in the relaxation of vascular smooth muscle. By activating sGC and increasing cGMP levels, NO triggers the activation of PKG, which modulates calcium handling, reduces calcium sensitivity, and promotes potassium efflux. These mechanisms collectively lower cytosolic calcium concentration and decrease the contractile state of the muscle, leading to vasodilation and improved blood flow. Understanding this pathway is essential for appreciating the physiological regulation of vascular tone and for developing therapeutic strategies targeting vascular disorders.
Pantoprazole and Muscle Cramps: Understanding Potential Side Effects
You may want to see also
Explore related products



![Vascular Smooth Muscle in Culture: Volume I and Volume II [2 volume set]](https://m.media-amazon.com/images/I/71CyD2g65BL._AC_UL320_.jpg)


![]()
Prostaglandins and EDHF: Vasodilatory prostaglandins and EDHF hyperpolarize membranes, decreasing calcium influx
Prostaglandins and endothelium-derived hyperpolarizing factor (EDHF) play crucial roles in the relaxation of vascular smooth muscle by modulating membrane potential and calcium influx. Vasodilatory prostaglandins, such as PGI₂ (prostacyclin) and PGE₂, are synthesized by the endothelium and act on specific receptors on smooth muscle cells. These prostaglandins activate G protein-coupled receptors linked to adenylate cyclase, increasing intracellular cyclic AMP (cAMP) levels. Elevated cAMP, in turn, activates protein kinase A (PKA), which phosphorylates target proteins, leading to the opening of potassium channels and hyperpolarization of the cell membrane. This hyperpolarization reduces the driving force for calcium entry through voltage-gated calcium channels, thereby decreasing intracellular calcium concentration and promoting smooth muscle relaxation.
EDHF functions as another key endothelial-derived factor that contributes to vascular smooth muscle relaxation, particularly in resistance arteries where nitric oxide (NO) and prostaglandins may be less dominant. EDHF acts by directly hyperpolarizing smooth muscle cells, a process mediated through the release of potassium ions from endothelial cells or by activating endothelial intermediate-conductance calcium-activated potassium channels (KCa3.1). The resulting efflux of potassium ions from endothelial cells creates a hyperpolarizing current that spreads to adjacent smooth muscle cells via myoendothelial gap junctions. This hyperpolarization of smooth muscle membranes reduces the openness of voltage-gated calcium channels, decreasing calcium influx and leading to muscle relaxation.
The interplay between prostaglandins and EDHF in vascular smooth muscle relaxation is particularly notable in conditions where NO bioavailability is compromised. For instance, in hypertension or diabetes, where NO production may be impaired, prostaglandins and EDHF become more prominent in mediating vasodilation. Prostaglandins, through their cAMP-dependent mechanisms, and EDHF, through direct hyperpolarization, provide alternative pathways to ensure adequate vascular relaxation. This redundancy highlights the importance of these factors in maintaining vascular homeostasis under various physiological and pathological conditions.
Mechanistically, the hyperpolarization induced by both prostaglandins and EDHF is critical for reducing calcium influx, which is essential for smooth muscle contraction. Intracellular calcium binds to calmodulin, activating myosin light chain kinase (MLCK) and initiating the contractile process. By decreasing calcium entry, prostaglandins and EDHF effectively inhibit this pathway, promoting relaxation. Additionally, the hyperpolarization caused by these factors can activate calcium-activated potassium channels (KCa channels) in smooth muscle cells, further enhancing membrane hyperpolarization and reinforcing the relaxation response.
In summary, vasodilatory prostaglandins and EDHF induce vascular smooth muscle relaxation by hyperpolarizing cell membranes, which subsequently decreases calcium influx. Prostaglandins achieve this through cAMP-dependent activation of potassium channels, while EDHF acts via direct hyperpolarization mechanisms involving potassium efflux and gap junction communication. Together, these factors ensure robust vasodilation, particularly in scenarios where NO is less effective. Understanding these pathways is essential for appreciating the complexity of vascular regulation and for developing therapeutic strategies targeting vascular dysfunction.
Why Do Muscle Cramps Occur During Illness? Causes and Remedies
You may want to see also
Explore related products





![]()
Adenosine Receptor Activation: Adenosine binds receptors, increases cAMP, reduces calcium, induces relaxation
Adenosine receptor activation plays a pivotal role in the relaxation of vascular smooth muscle, a process critical for regulating blood flow and vascular tone. When adenosine binds to its specific receptors on the surface of vascular smooth muscle cells, it initiates a cascade of intracellular events that ultimately lead to muscle relaxation. The primary receptors involved in this process are the A2A and A2B adenosine receptors, which are G protein-coupled receptors. Upon activation, these receptors stimulate the production of cyclic adenosine monophosphate (cAMP), a key second messenger in cellular signaling. The increase in cAMP levels is a direct consequence of adenosine binding and is essential for the subsequent steps in the relaxation pathway.
The elevation of cAMP activates protein kinase A (PKA), an enzyme that phosphorylates various target proteins within the cell. One of the critical targets of PKA is the phosphorylation of specific calcium channels and proteins involved in calcium regulation. This phosphorylation leads to a reduction in intracellular calcium concentration. Calcium is a crucial ion in muscle contraction, as it binds to calmodulin and activates myosin light-chain kinase (MLCK), which phosphorylates the myosin light chains and enables muscle contraction. By reducing calcium levels, adenosine receptor activation effectively inhibits this contractile pathway.
The decrease in intracellular calcium concentration is a key mechanism by which adenosine induces vascular smooth muscle relaxation. With less calcium available to activate the contractile machinery, the muscle cells transition from a contracted to a relaxed state. This relaxation is further supported by the simultaneous activation of myosin light-chain phosphatase (MLCP), which dephosphorylates the myosin light chains, counteracting the effects of MLCK. The combined actions of reduced calcium and increased MLCP activity ensure that the smooth muscle remains in a relaxed state, promoting vasodilation.
Additionally, the adenosine-induced increase in cAMP and subsequent PKA activation can also modulate other signaling pathways that contribute to relaxation. For instance, PKA may phosphorylate and inhibit Rho-kinase, a protein that enhances calcium sensitivity and promotes contraction. By inhibiting Rho-kinase, adenosine further reduces the contractile tone of vascular smooth muscle. This multifaceted approach ensures that adenosine receptor activation is a potent and effective mechanism for inducing vascular relaxation.
In summary, adenosine receptor activation triggers a well-coordinated series of events that lead to vascular smooth muscle relaxation. From the initial binding of adenosine to its receptors, through the increase in cAMP and activation of PKA, to the reduction in intracellular calcium and modulation of contractile proteins, each step is crucial for achieving the desired physiological effect. Understanding this mechanism not only highlights the importance of adenosine in vascular regulation but also provides insights into potential therapeutic targets for conditions involving abnormal vascular tone.
Flu Symptoms: Sore Muscles and Sensitivity to Cold
You may want to see also
Explore related products




$186.91 $219.99


![]()
Acetylcholine and M3 Receptors: Acetylcholine activates M3 receptors, increases cAMP, promotes relaxation
Acetylcholine (ACh) plays a significant role in the relaxation of vascular smooth muscle through its interaction with M3 muscarinic receptors. When acetylcholine binds to M3 receptors located on the surface of vascular smooth muscle cells, it initiates a signaling cascade that ultimately leads to muscle relaxation. This process is crucial in regulating blood vessel diameter and, consequently, blood flow. The activation of M3 receptors by acetylcholine is a key mechanism in vasodilation, which is essential for maintaining proper circulatory function.
Upon binding to M3 receptors, acetylcholine triggers the activation of G proteins, specifically the Gq subtype. This activation stimulates the enzyme phospholipase C (PLC), which hydrolyzes phosphatidylinositol 4,5-bisphosphate (PIP2) into inositol trisphosphate (IP3) and diacylglycerol (DAG). IP3 acts as a second messenger by binding to IP3 receptors on the endoplasmic reticulum, leading to the release of calcium ions (Ca²⁺) into the cytoplasm. While calcium is often associated with muscle contraction, the subsequent steps in this pathway promote relaxation.
The increase in cytoplasmic calcium concentration activates calcium-sensitive enzymes, including adenylate cyclase. This enzyme catalyzes the conversion of adenosine triphosphate (ATP) to cyclic adenosine monophosphate (cAMP). Elevated levels of cAMP are a critical factor in promoting vascular smooth muscle relaxation. cAMP activates protein kinase A (PKA), which phosphorylates various target proteins, including those involved in the regulation of calcium channels and contractile filaments. This phosphorylation reduces the sensitivity of the muscle to calcium, thereby inhibiting contraction and promoting relaxation.
Additionally, the activation of M3 receptors and the subsequent increase in cAMP levels lead to the inhibition of myosin light chain kinase (MLCK). MLCK is responsible for phosphorylating the myosin light chains, a process essential for muscle contraction. By inhibiting MLCK, the pathway reduces the phosphorylation of myosin light chains, which disrupts the interaction between actin and myosin filaments. This disruption results in the relaxation of vascular smooth muscle cells, allowing blood vessels to dilate.
In summary, acetylcholine-induced activation of M3 receptors initiates a complex signaling pathway that ultimately promotes vascular smooth muscle relaxation. Through the increase in cAMP levels and the subsequent activation of PKA, the pathway reduces calcium sensitivity and inhibits contractile mechanisms. This process is vital for regulating blood vessel tone and ensuring adequate blood flow to tissues. Understanding this mechanism provides valuable insights into the pharmacological and physiological regulation of vascular function, highlighting the importance of acetylcholine and M3 receptors in cardiovascular health.
Breathing and Muscles: The Surprising Link
You may want to see also
Explore related products






![]()
Calcium Channel Blockers: Block L-type calcium channels, reduce intracellular calcium, cause relaxation
Calcium channel blockers (CCBs) are a class of medications that play a crucial role in promoting vascular smooth muscle relaxation. Their primary mechanism of action involves selectively blocking L-type calcium channels, which are abundantly expressed in vascular smooth muscle cells. These channels are responsible for the influx of calcium ions (Ca²⁺) into the cell during membrane depolarization. By inhibiting these channels, CCCs effectively reduce the entry of calcium into the cytoplasm, thereby lowering intracellular calcium concentrations. This reduction in calcium is pivotal because calcium ions act as a key second messenger in the contraction process of smooth muscle cells. When intracellular calcium levels decrease, the calcium-dependent signaling pathways that trigger muscle contraction are disrupted, leading to relaxation of the vascular smooth muscle.
The relaxation induced by CCBs is particularly significant in blood vessels, where vascular smooth muscle tone regulates vessel diameter and, consequently, blood pressure. In vascular smooth muscle cells, calcium binds to calmodulin, activating myosin light-chain kinase (MLCK). MLCK phosphorylates the myosin light chains, enabling actin-myosin cross-bridge formation and muscle contraction. By blocking L-type calcium channels, CCBs limit the availability of calcium for this process, thereby inhibiting MLCK activation and reducing the phosphorylation of myosin light chains. This disruption prevents the contractile machinery from functioning effectively, resulting in smooth muscle relaxation and vasodilation. The vasodilatory effect of CCBs is essential in managing conditions like hypertension, where excessive vascular smooth muscle contraction contributes to elevated blood pressure.
Another critical aspect of CCBs is their ability to modulate calcium-dependent processes beyond direct contraction. Intracellular calcium also regulates the activity of other enzymes and signaling molecules involved in vascular tone maintenance. For instance, reduced calcium levels inhibit the activity of calcium-calmodulin-dependent protein kinase II (CaMKII), which plays a role in sustaining vascular smooth muscle contraction. Additionally, lower calcium concentrations can activate calcium-sensitive potassium channels, leading to hyperpolarization of the cell membrane and further relaxation. These secondary mechanisms amplify the relaxing effect of CCBs, ensuring a robust and sustained reduction in vascular smooth muscle tone.
Clinically, CCBs are widely used to treat hypertension and angina due to their potent vasodilatory effects. By relaxing vascular smooth muscle, they decrease peripheral resistance, which reduces the workload on the heart and lowers blood pressure. The specificity of CCBs for L-type calcium channels minimizes their impact on other cell types, such as cardiac muscle, where T-type calcium channels predominate. However, their use must be carefully monitored, as excessive vasodilation can lead to reflex tachycardia or hypotension. Despite these considerations, CCBs remain a cornerstone therapy for conditions requiring vascular smooth muscle relaxation, highlighting their importance in cardiovascular medicine.
In summary, calcium channel blockers induce vascular smooth muscle relaxation by selectively blocking L-type calcium channels, thereby reducing intracellular calcium levels. This inhibition disrupts calcium-dependent contraction pathways, including MLCK activation and myosin light-chain phosphorylation, while also modulating secondary calcium-sensitive mechanisms. The resulting vasodilation is therapeutically valuable for managing hypertension and related conditions. Understanding the precise mechanism of CCBs underscores their efficacy and reinforces their role as a key pharmacological tool in promoting vascular smooth muscle relaxation.
Understanding Hand Muscle Twitch Causes: Triggers and Remedies Explained
You may want to see also
Frequently asked questions
Nitric oxide (NO) is a key vasodilator produced by endothelial cells. It diffuses into vascular smooth muscle cells, where it activates guanylate cyclase, increasing cyclic GMP (cGMP) levels. This leads to decreased intracellular calcium, causing relaxation of the smooth muscle and vasodilation.
Calcium channel blockers (e.g., nifedipine) inhibit voltage-gated calcium channels in vascular smooth muscle cells. By reducing calcium influx, they lower intracellular calcium levels, preventing muscle contraction and promoting relaxation.
Prostacyclin (PGI2) is a vasodilator produced by endothelial cells. It binds to IP receptors on smooth muscle cells, activating adenylate cyclase and increasing cyclic AMP (cAMP). This reduces calcium sensitivity, leading to muscle relaxation and vasodilation.
Activation of beta-2 adrenergic receptors by catecholamines (e.g., epinephrine) stimulates adenylate cyclase, increasing cAMP levels. This activates protein kinase A (PKA), which reduces calcium release and sensitivity, resulting in smooth muscle relaxation.
Opening of potassium channels in vascular smooth muscle cells leads to hyperpolarization of the cell membrane. This reduces the opening of voltage-gated calcium channels, decreasing calcium influx and promoting muscle relaxation.































