Chronic muscle pain, a persistent and often debilitating condition, can arise from a variety of factors, including overuse injuries, poor posture, and repetitive strain. Conditions such as fibromyalgia, myofascial pain syndrome, and chronic fatigue syndrome are also known to cause widespread muscle discomfort. Additionally, underlying medical issues like autoimmune disorders, infections, or metabolic imbalances can contribute to ongoing pain. Lifestyle factors, including stress, lack of physical activity, and inadequate sleep, may exacerbate symptoms, while nutritional deficiencies or dehydration can further weaken muscles. Understanding the root causes of chronic muscle pain is essential for developing effective treatment plans and improving quality of life.
Explore related products






What You'll Learn
- Fibromyalgia: Widespread pain, fatigue, and tender points without inflammation or tissue damage
- Myofascial Pain Syndrome: Trigger points in muscles causing localized pain and referred discomfort
- Polymyalgia Rheumatica: Inflammatory condition causing muscle pain, stiffness, especially in shoulders and hips
- Chronic Fatigue Syndrome: Persistent fatigue, muscle pain, and post-exertional malaise with no clear cause
- Statin-Induced Myopathy: Muscle pain and weakness caused by cholesterol-lowering statin medications
![]()
Fibromyalgia: Widespread pain, fatigue, and tender points without inflammation or tissue damage
Fibromyalgia is a complex and chronic condition characterized primarily by widespread musculoskeletal pain, fatigue, and specific tender points throughout the body. Unlike conditions such as arthritis, fibromyalgia does not cause inflammation or tissue damage, yet the pain it produces can be debilitating. The exact cause of fibromyalgia remains unknown, but it is believed to involve a combination of genetic, environmental, and neurological factors. Individuals with fibromyalgia often experience heightened sensitivity to pain due to abnormalities in how the brain and spinal cord process pain signals, a phenomenon known as central sensitization. This means that even mild stimuli can be perceived as intensely painful.
The widespread pain associated with fibromyalgia is not limited to muscles but can affect joints, tendons, and other soft tissues. Patients frequently describe the pain as a constant, deep ache that persists throughout the day and may worsen with physical activity, stress, or changes in weather. Alongside pain, fatigue is a hallmark symptom, often described as a profound exhaustion that is not relieved by rest. This fatigue can significantly impair daily functioning, making it difficult for individuals to perform routine tasks or maintain regular work schedules. Sleep disturbances, such as difficulty falling asleep or staying asleep, are also common and can exacerbate both pain and fatigue.
Tender points are another defining feature of fibromyalgia. These are specific areas on the body that are highly sensitive to pressure, even when applied with minimal force. Common tender points include the back of the head, shoulders, chest, elbows, hips, and knees. During a physical examination, a healthcare provider may apply pressure to these points to assess their tenderness. However, it is important to note that the presence of tender points alone is not sufficient for a fibromyalgia diagnosis, as other symptoms and criteria must also be met.
Diagnosing fibromyalgia can be challenging due to the absence of visible inflammation or tissue damage and the lack of specific laboratory tests. Healthcare providers typically rely on a combination of patient history, physical examination, and the exclusion of other conditions that could explain the symptoms. The American College of Rheumatology has established diagnostic criteria that include widespread pain lasting at least three months and the presence of other symptoms such as fatigue, cognitive difficulties (often referred to as "fibro fog"), and sleep disturbances. Early diagnosis is crucial, as it allows for the implementation of management strategies to improve quality of life.
Management of fibromyalgia focuses on alleviating symptoms and improving overall function. A multidisciplinary approach is often most effective, incorporating medications, physical therapy, exercise, and lifestyle modifications. Medications such as antidepressants, anti-seizure drugs, and pain relievers may be prescribed to address pain, fatigue, and sleep issues. Regular, low-impact exercise, such as walking, swimming, or yoga, can help reduce pain and improve mobility. Cognitive-behavioral therapy (CBT) and stress management techniques are also valuable tools for coping with the emotional and psychological aspects of the condition. Patients are encouraged to work closely with their healthcare team to develop a personalized treatment plan tailored to their specific needs.
Antibiotics and Muscle Cramps: Is There a Link?
You may want to see also
Explore related products




![]()
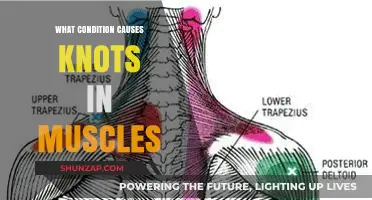
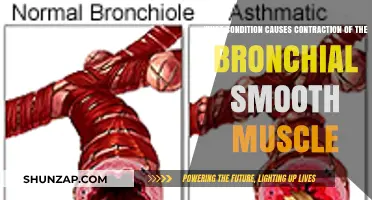
Myofascial Pain Syndrome: Trigger points in muscles causing localized pain and referred discomfort
Myofascial Pain Syndrome (MPS) is a chronic condition characterized by the presence of trigger points in muscles, which cause localized pain and referred discomfort. These trigger points are hyperirritable spots within taut bands of skeletal muscle or fascia, often arising from overuse, injury, or stress. When pressure is applied to these points, it not only elicits pain at the site but also refers pain to other areas of the body, sometimes distant from the origin. This referred pain is a hallmark of MPS and can be misleading, as individuals may experience symptoms in regions unrelated to the actual trigger point. Understanding the mechanism of trigger points is crucial for diagnosing and managing this condition effectively.
The development of trigger points in MPS is often linked to sustained muscle tension, poor posture, repetitive motions, or direct trauma. For instance, individuals who sit for prolonged periods with poor ergonomics may develop trigger points in the neck, shoulders, or lower back. Similarly, athletes or workers engaging in repetitive activities are at higher risk due to the continuous strain on specific muscle groups. Psychological factors, such as stress and anxiety, can also contribute by causing involuntary muscle tension. Identifying and addressing these underlying causes is essential in preventing the progression of MPS and reducing the frequency of flare-ups.
Diagnosing MPS involves a thorough physical examination to locate trigger points and assess their referral patterns. Healthcare providers often use palpation to identify taut bands and tender spots within the muscles. Additionally, patients may be asked to describe the nature and location of their pain, as well as any activities that exacerbate or alleviate symptoms. While imaging tests like MRI or ultrasound are not typically used for diagnosis, they may be employed to rule out other conditions with similar symptoms, such as herniated discs or nerve entrapments.
Treatment for MPS is multifaceted and aims to deactivate trigger points, alleviate pain, and restore normal muscle function. Manual therapies, such as massage, myofascial release, and dry needling, are commonly used to target trigger points directly. Stretching and strengthening exercises prescribed by physical therapists can help improve muscle flexibility and reduce tension. Heat therapy, ultrasound, and transcutaneous electrical nerve stimulation (TENS) may also provide symptomatic relief. In some cases, medications like muscle relaxants, anti-inflammatory drugs, or local anesthetics are used to manage pain and inflammation.
Preventing recurrence of MPS involves lifestyle modifications and ergonomic adjustments. Patients are often advised to maintain proper posture, take regular breaks during prolonged activities, and incorporate stress management techniques like mindfulness or yoga. Educating individuals about body mechanics and the importance of balanced muscle use can significantly reduce the risk of developing new trigger points. By combining targeted treatments with proactive self-care, individuals with MPS can achieve long-term relief and improve their quality of life.
Rib Cage Muscle Spasms: A Hidden Cause of Shortness of Breath?
You may want to see also
Explore related products






![]()
Polymyalgia Rheumatica: Inflammatory condition causing muscle pain, stiffness, especially in shoulders and hips
Polymyalgia Rheumatica (PMR) is a systemic inflammatory disorder that predominantly affects individuals over the age of 50, causing chronic muscle pain and stiffness, particularly in the shoulders and hips. This condition is characterized by an inflammatory response that targets the synovial membranes and soft tissues around the joints, leading to significant discomfort and reduced mobility. The pain associated with PMR is often described as aching, throbbing, or stiff, and it is typically worse in the morning or after periods of inactivity. Patients may also experience systemic symptoms such as fatigue, fever, weight loss, and a general sense of malaise, which can further impact their quality of life.
The exact cause of Polymyalgia Rheumatica remains unknown, but it is believed to involve a combination of genetic, environmental, and immune system factors. Research suggests that an abnormal immune response plays a central role, where the body’s immune system mistakenly attacks healthy tissues, leading to inflammation. This condition is closely associated with giant cell arteritis (GCA), another inflammatory disorder that affects the blood vessels, particularly the arteries in the head and neck. In fact, up to 15% of PMR patients may also develop GCA, emphasizing the need for careful monitoring and evaluation of vascular symptoms such as headaches, jaw pain, or vision changes.
Diagnosing PMR relies on a combination of clinical symptoms, physical examination, and laboratory tests, as there is no single definitive test for the condition. Elevated levels of inflammatory markers, such as erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP), are commonly observed in PMR patients. Imaging studies like ultrasound or magnetic resonance imaging (MRI) may also reveal inflammation in the affected areas, particularly the shoulder and hip girdles. Early diagnosis is crucial, as prompt treatment can significantly alleviate symptoms and prevent complications.
Treatment for Polymyalgia Rheumatica primarily involves the use of corticosteroids, such as prednisone, which are highly effective in reducing inflammation and relieving pain and stiffness. The dosage and duration of treatment are tailored to individual needs, with most patients experiencing rapid improvement within days of starting therapy. However, long-term use of corticosteroids can lead to side effects such as osteoporosis, weight gain, and increased infection risk, necessitating careful monitoring and management. In some cases, additional medications or physical therapy may be recommended to support recovery and maintain joint function.
Living with PMR requires a proactive approach to managing symptoms and maintaining overall health. Patients are encouraged to stay physically active, as gentle exercises can help improve flexibility, strength, and range of motion. A balanced diet rich in anti-inflammatory foods, such as fruits, vegetables, and omega-3 fatty acids, may also support symptom management. Regular follow-ups with a rheumatologist are essential to monitor disease activity, adjust treatment as needed, and address any concerns or complications. With appropriate care, most individuals with PMR can achieve significant relief and resume their daily activities.
Opioids and Muscle Twitching: What's the Connection?
You may want to see also
Explore related products






![]()
Chronic Fatigue Syndrome: Persistent fatigue, muscle pain, and post-exertional malaise with no clear cause
Chronic Fatigue Syndrome (CFS), also known as Myalgic Encephalomyelitis (ME), is a complex and debilitating condition characterized by persistent fatigue, muscle pain, and post-exertional malaise (PEM) without a clear underlying cause. Unlike typical fatigue or muscle soreness, which improve with rest, the symptoms of CFS are chronic, often worsening after physical or mental exertion. This condition significantly impairs daily functioning and quality of life, yet its etiology remains poorly understood. While the exact cause of CFS is unknown, research suggests it may involve a combination of factors, including viral infections, immune system dysfunction, hormonal imbalances, and genetic predisposition. The muscle pain experienced by individuals with CFS is often widespread and may be accompanied by joint pain, further complicating diagnosis and treatment.
Persistent fatigue in CFS is not alleviated by rest and is often described as profound and unrelenting. It is distinct from the fatigue experienced in other conditions, as it can be exacerbated by even minimal physical or cognitive activity. This fatigue is a core symptom and is often accompanied by muscle pain, which can be migratory and affect different muscle groups over time. The pain is typically described as aching or soreness and may be severe enough to interfere with mobility and daily activities. Post-exertional malaise, another hallmark of CFS, refers to a worsening of symptoms after physical, mental, or emotional exertion, often delayed by hours or days. This symptom underscores the need for careful activity management, as overexertion can lead to prolonged symptom flares.
The absence of a clear cause for CFS poses significant challenges for both patients and healthcare providers. Diagnostic criteria, such as the CDC’s 1994 definition or the more recent Canadian Consensus Criteria, rely on symptom presentation and exclusion of other conditions. Common differential diagnoses include fibromyalgia, autoimmune disorders, and mental health conditions like depression. However, unlike these conditions, CFS is characterized by the unique combination of persistent fatigue, muscle pain, and post-exertional malaise. Laboratory tests are often unremarkable, further complicating the diagnostic process. This lack of objective biomarkers can lead to skepticism and misunderstanding, emphasizing the need for increased awareness and research into the condition.
Management of CFS focuses on symptom relief and improving quality of life, as there is currently no cure. Treatment strategies are individualized and may include pacing, a technique to balance activity and rest to avoid post-exertional malaise. Physical therapy, particularly graded exercise therapy (GET), must be approached cautiously, as aggressive exercise can exacerbate symptoms. Medications such as pain relievers, sleep aids, and antidepressants may be used to address specific symptoms. Cognitive-behavioral therapy (CBT) can help patients cope with the psychological impact of living with a chronic illness. Lifestyle modifications, such as stress management and dietary adjustments, may also provide some relief. Patient education and support from healthcare providers are crucial in navigating the complexities of CFS.
The impact of CFS extends beyond physical symptoms, often affecting emotional and social well-being. Many individuals with CFS face challenges in maintaining employment, relationships, and social activities due to the unpredictability and severity of their symptoms. Stigma and lack of understanding from others can exacerbate feelings of isolation and frustration. Advocacy efforts are essential to raise awareness, improve healthcare provider education, and fund research into the underlying mechanisms and potential treatments for CFS. Until more definitive answers are found, a multidisciplinary approach that addresses the physical, emotional, and social aspects of the condition remains the cornerstone of care for individuals living with Chronic Fatigue Syndrome.
Metoprolol and Muscle Spasms: What's the Link?
You may want to see also
Explore related products






![]()
Statin-Induced Myopathy: Muscle pain and weakness caused by cholesterol-lowering statin medications
Statin-induced myopathy is a well-documented condition characterized by muscle pain and weakness resulting from the use of cholesterol-lowering statin medications. Statins, such as atorvastatin, simvastatin, and rosuvastatin, are widely prescribed to reduce LDL cholesterol and lower the risk of cardiovascular disease. However, in some individuals, these medications can lead to musculoskeletal symptoms ranging from mild discomfort to severe, debilitating pain. The exact mechanism behind statin-induced myopathy is not fully understood, but it is believed to involve impaired muscle cell energy production, oxidative stress, and damage to muscle fibers. This condition is a significant concern, as it can affect a patient’s quality of life and adherence to necessary lipid-lowering therapy.
The symptoms of statin-induced myopathy typically include muscle pain (myalgia), tenderness, stiffness, and generalized weakness, often affecting the proximal muscle groups of the limbs. In more severe cases, patients may develop myositis (muscle inflammation) or rhabdomyolysis, a life-threatening condition where muscle tissue breaks down rapidly, releasing harmful proteins into the bloodstream. Risk factors for developing statin-induced myopathy include higher statin dosages, older age, female sex, renal impairment, and concurrent use of medications that interact with statins, such as fibrates or certain antibiotics. Genetic predisposition, particularly variations in the SLCO1B1 gene, has also been linked to increased susceptibility.
Diagnosing statin-induced myopathy involves a careful clinical evaluation, including a detailed medical history and physical examination. Laboratory tests, such as measuring creatine kinase (CK) levels, are often performed to assess muscle damage. Elevated CK levels, particularly if they are more than 10 times the upper limit of normal, suggest severe myopathy or rhabdomyolysis. However, it is important to note that many patients with statin-induced myalgia have normal CK levels, making the diagnosis reliant on symptom correlation with statin use. Excluding other causes of muscle pain, such as hypothyroidism, electrolyte imbalances, or autoimmune disorders, is also crucial.
Management of statin-induced myopathy primarily involves discontinuing or reducing the dose of the offending statin. In many cases, symptoms resolve within weeks after stopping the medication. For patients who require lipid-lowering therapy but cannot tolerate their current statin, switching to a different statin or an alternative medication, such as ezetimibe or PCSK9 inhibitors, may be considered. Coenzyme Q10 supplementation has been proposed as a potential adjunctive therapy, although evidence supporting its efficacy is limited. Patients should be closely monitored for recurrence of symptoms if statins are reintroduced, often at a lower dose or with a different formulation.
Preventing statin-induced myopathy involves careful patient selection and monitoring. Clinicians should assess individual risk factors before initiating statin therapy and consider starting with lower doses, especially in high-risk populations. Regular follow-up appointments to evaluate tolerability and monitor for muscle symptoms are essential. Patient education is also critical, as recognizing early signs of myopathy can prevent progression to more severe complications. While statins remain a cornerstone of cardiovascular disease prevention, balancing their benefits against the risk of myopathy is vital for optimal patient care.
In summary, statin-induced myopathy is a significant cause of chronic muscle pain and weakness in individuals taking cholesterol-lowering statin medications. Understanding its clinical presentation, risk factors, and management strategies is essential for healthcare providers to address this condition effectively. By adopting a proactive approach to patient care, clinicians can minimize the impact of statin-induced myopathy while ensuring patients continue to receive the cardiovascular benefits of lipid-lowering therapy.
Holding Urine: Straining Your Muscles and Bladder
You may want to see also
Frequently asked questions
Common conditions include fibromyalgia, myofascial pain syndrome, chronic fatigue syndrome, and autoimmune disorders like lupus or rheumatoid arthritis.
Yes, prolonged stress and anxiety can lead to muscle tension and chronic pain due to increased cortisol levels and persistent muscle tightness.
Poor posture places uneven stress on muscles, leading to strain, imbalances, and chronic pain, especially in the neck, back, and shoulders.
Yes, repetitive strain injuries, overuse from physical activity, or trauma can lead to chronic muscle pain if not properly treated or rehabilitated.