The relaxation of smooth muscle in both coronary and systemic vasculature is a critical physiological process that regulates blood flow and blood pressure. One of the most well-known drugs that effectively achieves this is nitroglycerin, a nitrate derivative that acts as a vasodilator. Nitroglycerin works by releasing nitric oxide (NO), which activates guanylate cyclase in smooth muscle cells, leading to increased cyclic guanosine monophosphate (cGMP) levels. This, in turn, causes relaxation of the smooth muscle in blood vessel walls, reducing vascular resistance and improving blood flow. Nitroglycerin is widely used in the treatment of angina pectoris and hypertension due to its potent effects on both coronary and systemic vasculature, making it a cornerstone in cardiovascular therapy.
Explore related products






What You'll Learn
![]()
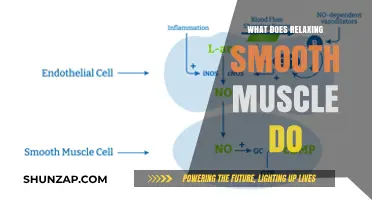
Nitrates mechanism of action
Nitrates, such as nitroglycerin, are a cornerstone in the management of angina pectoris and acute coronary syndromes due to their potent vasodilatory effects. Their mechanism of action hinges on the release of nitric oxide (NO), a key signaling molecule that activates soluble guanylate cyclase in smooth muscle cells. This enzyme catalyzes the conversion of guanosine triphosphate (GTP) to cyclic guanosine monophosphate (cGMP), which subsequently activates protein kinase G. The resultant phosphorylation of target proteins leads to dephosphorylation of myosin light chains, causing relaxation of smooth muscle in both venous and arterial vasculature. This dual action reduces preload and afterload on the heart, thereby decreasing myocardial oxygen demand and alleviating ischemia.
To maximize the efficacy of nitrates, it is crucial to understand their pharmacokinetics and administration routes. Sublingual nitroglycerin, for instance, acts within 1–3 minutes and lasts 20–40 minutes, making it ideal for acute angina relief. Dosage typically starts at 0.4 mg, with repeat doses every 5 minutes up to three times, if needed. Prolonged use, however, can lead to tolerance due to nitrate-induced oxidative stress depleting endogenous NO stores. To mitigate this, clinicians often prescribe intermittent dosing (e.g., 12 hours on, 12 hours off) or adjunctive therapies like phosphodiesterase-5 inhibitors.
A comparative analysis of nitrates versus other vasodilators highlights their unique advantages. Unlike calcium channel blockers, which primarily target arterial smooth muscle, nitrates affect both venous and arterial systems, offering a more balanced reduction in cardiac workload. However, their rapid tolerance development and potential for severe hypotension, especially in volume-depleted patients, necessitate cautious use. For elderly patients or those with comorbidities, starting with lower doses (e.g., 0.3 mg sublingually) and monitoring for orthostatic hypotension is advisable.
Practically, patients should be educated on proper storage and administration techniques. Nitroglycerin tablets should be stored in amber vials to protect from light degradation and kept at room temperature. Patients must avoid swallowing the tablet, as this reduces bioavailability and delays onset. Additionally, concurrent use of phosphodiesterase-5 inhibitors (e.g., sildenafil) is contraindicated due to the risk of severe hypotension. For chronic management, transdermal patches or long-acting oral formulations can be considered, but these require careful titration to avoid tolerance and adverse effects.
In conclusion, nitrates’ mechanism of action—centered on NO-mediated smooth muscle relaxation—makes them indispensable in cardiovascular care. Their ability to reduce preload and afterload provides rapid symptomatic relief, but their limitations, such as tolerance and hypotension, demand strategic use. By adhering to dosing guidelines, monitoring for adverse effects, and educating patients, clinicians can optimize nitrate therapy to improve outcomes in coronary and systemic vascular conditions.
Is Percocet a Muscle Relaxer? Understanding Its Uses and Effects
You may want to see also
Explore related products






![]()
Calcium channel blockers effects
Calcium channel blockers (CCBs) are a cornerstone in the management of cardiovascular conditions, primarily due to their ability to relax smooth muscle in both coronary and systemic vasculature. By inhibiting calcium influx into vascular smooth muscle cells, CCBs reduce vascular resistance, improve blood flow, and decrease myocardial oxygen demand. This mechanism makes them particularly effective in treating hypertension, angina, and certain arrhythmias. For instance, drugs like amlodipine, nifedipine, and verapamil are widely prescribed, with dosages typically ranging from 5 to 10 mg daily for amlodipine and 30 to 60 mg extended-release for nifedipine, depending on patient age and comorbidities.
One of the most significant effects of CCBs is their vasodilatory action, which directly addresses the question of what drug relaxes smooth muscle in coronary and systemic vasculature. By dilating blood vessels, CCBs lower blood pressure and reduce the workload on the heart. This is particularly beneficial for elderly patients with hypertension, as CCBs are often better tolerated than other antihypertensive agents like beta-blockers, which can exacerbate bradycardia or asthma. However, caution is advised in patients with severe aortic stenosis or heart failure, as excessive vasodilation can lead to hypotension or worsen cardiac output.
CCBs also exhibit coronary vasodilation, making them valuable in managing angina pectoris. By relaxing coronary smooth muscle, they improve oxygen supply to the myocardium, alleviating chest pain. For example, diltiazem and verapamil, both non-dihydropyridine CCBs, are often used in patients with stable angina, with dosages starting at 120 mg daily for diltiazem and 180 mg daily for verapamil. These agents are particularly useful in patients with concomitant hypertension, as they address both conditions simultaneously. However, their negative inotropic effects necessitate careful monitoring in patients with compromised left ventricular function.
Beyond their cardiovascular benefits, CCBs have unique side effects that clinicians must consider. Dihydropyridine CCBs, such as amlodipine and nifedipine, are more likely to cause peripheral edema due to their potent arterial vasodilatory effects. This can be managed by adjusting dosage or adding a diuretic. Non-dihydropyridine CCBs, on the other hand, may cause constipation or bradycardia, requiring alternative agents in patients with gastrointestinal or conduction issues. Practical tips include taking CCBs with food to minimize gastrointestinal discomfort and avoiding abrupt discontinuation to prevent rebound hypertension.
In summary, calcium channel blockers are a versatile class of drugs that effectively relax smooth muscle in coronary and systemic vasculature, making them indispensable in cardiovascular therapy. Their ability to lower blood pressure, relieve angina, and improve blood flow is well-established, but their use requires careful patient selection and monitoring. By understanding their mechanisms, dosages, and side effects, clinicians can optimize their benefits while minimizing risks, ensuring better outcomes for patients with hypertension, angina, and related conditions.
Effective Techniques to Relax Tense Muscles and Ease Stress
You may want to see also
Explore related products





![]()
Direct vasodilators examples
Nitrates stand as a cornerstone in the treatment of angina and hypertension, acting as direct vasodilators that relax smooth muscle in both coronary and systemic vasculature. These compounds, including nitroglycerin, isosorbide dinitrate, and isosorbide mononitrate, release nitric oxide (NO), which activates guanylate cyclase, increasing cyclic GMP levels and leading to smooth muscle relaxation. Nitroglycerin, for instance, is commonly administered sublingually in doses of 0.3–0.6 mg for acute angina relief, with effects lasting 20–30 minutes. Its rapid onset makes it ideal for immediate symptom control, but tolerance can develop with frequent use, necessitating nitrate-free intervals.
In contrast to nitrates, calcium channel blockers (CCBs) like nifedipine and amlodipine offer a different mechanism of direct vasodilation. By inhibiting calcium influx into vascular smooth muscle cells, CCBs reduce contraction force, leading to relaxation and decreased peripheral resistance. Nifedipine, often prescribed in doses of 10–20 mg every 8 hours, is particularly effective for systemic hypertension and Raynaud’s phenomenon. However, its short half-life can cause reflex tachycardia, making extended-release formulations preferable for long-term management. Amlodipine, with a once-daily dose of 5–10 mg, provides smoother control and is better tolerated, especially in elderly patients.
Hydralazine, another direct vasodilator, works by relaxing arteriolar smooth muscle, primarily through mechanisms involving increased cyclic GMP and reduced calcium sensitivity. It is often used in combination with beta-blockers and diuretics for severe hypertension, particularly in pregnant women or patients with renal impairment. Dosage typically starts at 10 mg every 6 hours, titrated up to 50–100 mg daily based on response. While effective, hydralazine can cause reflex tachycardia and fluid retention, necessitating careful monitoring and adjunctive therapy.
Minoxidil, originally developed as an antihypertensive, is a potent direct vasodilator used primarily in severe, refractory hypertension. It acts by opening ATP-sensitive potassium channels in vascular smooth muscle, leading to hyperpolarization and relaxation. Dosage begins at 2.5 mg daily, increasing gradually to 40 mg or more if needed. Minoxidil’s efficacy comes with significant side effects, including fluid retention and hypertrichosis, making it a last-resort option. Patients require concurrent use of a diuretic and beta-blocker to mitigate adverse effects.
Among newer agents, sodium nitroprusside remains a critical intravenous vasodilator for hypertensive emergencies, such as postoperative hypertension or acute heart failure. It releases NO directly, causing rapid and profound vasodilation. Administered as a continuous infusion starting at 0.25 mcg/kg/min, the dose is titrated to achieve the desired blood pressure reduction. Its short half-life allows for precise control, but continuous monitoring is essential due to risks of cyanide toxicity with prolonged use. This agent is reserved for intensive care settings due to its narrow therapeutic window.
In practice, selecting a direct vasodilator requires balancing efficacy, side effects, and patient-specific factors. Nitrates are ideal for acute coronary syndromes, CCBs for long-term hypertension management, and hydralazine or minoxidil for resistant cases. Sodium nitroprusside serves as a lifesaving option in emergencies. Each drug’s mechanism, dosage, and potential complications underscore the importance of tailored therapy, emphasizing the need for clinical judgment and patient education to optimize outcomes.
Naproxen and Muscle Relaxers: Safe Combination or Risky Mix?
You may want to see also
Explore related products






![]()
Endothelial-derived factors role
The endothelium, a single-cell layer lining blood vessels, is not merely a passive barrier but an active regulator of vascular tone. It secretes a myriad of factors that influence smooth muscle relaxation, a critical process for maintaining blood flow in both coronary and systemic vasculature. Among these, nitric oxide (NO) stands out as a key player. Produced by endothelial nitric oxide synthase (eNOS), NO diffuses into adjacent smooth muscle cells, where it activates guanylate cyclase, increases cyclic guanosine monophosphate (cGMP), and ultimately leads to vasodilation. This mechanism is central to the action of drugs like nitrates (e.g., nitroglycerin) and phosphodiesterase-5 inhibitors (e.g., sildenafil), which either directly donate NO or enhance its signaling pathway.
Consider the clinical application of nitroglycerin, a cornerstone in managing angina pectoris. When administered sublingually at a dose of 0.3–0.6 mg, it rapidly metabolizes to release NO, dilating coronary arteries and reducing myocardial oxygen demand. However, its systemic vasodilatory effects can cause reflex tachycardia and hypotension, underscoring the delicate balance of endothelial-derived factors in vascular regulation. For older adults or patients with comorbidities, starting with the lowest effective dose and monitoring blood pressure is essential to avoid adverse effects.
Beyond NO, prostacyclin (PGI2) is another endothelial-derived factor critical for vascular homeostasis. Synthesized from arachidonic acid via cyclooxygenase (COX), PGI2 binds to IP receptors on smooth muscle cells, elevating cAMP and promoting relaxation. Drugs like epoprostenol, a synthetic PGI2 analog, are used in pulmonary arterial hypertension to dilate systemic and pulmonary vessels. Administered intravenously at doses titrated to effect (typically starting at 2 ng/kg/min), it requires careful monitoring due to its potent vasodilatory and potential hypotensive effects. This highlights the importance of endothelial prostanoid pathways in therapeutic interventions.
A comparative analysis reveals that while NO and PGI2 both induce vasodilation, their mechanisms and clinical applications differ. NO acts rapidly and is more localized, making it ideal for acute coronary syndromes, whereas PGI2 has a broader systemic effect, suited for chronic conditions like pulmonary hypertension. Endothelin-1 (ET-1), another endothelial-derived factor, paradoxically promotes vasoconstriction, and its antagonists (e.g., bosentan) are used to counteract excessive ET-1 activity in conditions like pulmonary hypertension. This duality underscores the endothelium’s complex role in vascular tone regulation.
In practice, understanding endothelial-derived factors allows clinicians to tailor therapies to specific vascular conditions. For instance, combining NO donors with statins, which upregulate eNOS expression, can enhance vasodilatory effects in atherosclerotic patients. Conversely, avoiding nonsteroidal anti-inflammatory drugs (NSAIDs) in patients on PGI2 therapy prevents COX inhibition and maintains prostacyclin production. Such nuanced approaches, grounded in endothelial biology, optimize outcomes while minimizing risks. By leveraging these factors, clinicians can effectively manage vascular disorders with precision and efficacy.
Tearing Muscles to Relax: Fact or Fiction? Unraveling the Myth
You may want to see also
Explore related products




![]()
Phosphodiesterase inhibitors impact
Phosphodiesterase (PDE) inhibitors are a class of drugs that play a pivotal role in relaxing smooth muscle in both coronary and systemic vasculature by enhancing the effects of cyclic nucleotides, primarily cyclic adenosine monophosphate (cAMP) and cyclic guanosine monophosphate (cGMP). These enzymes, which degrade these second messengers, are inhibited by PDE inhibitors, leading to vasodilation, improved blood flow, and reduced vascular resistance. Among the most well-known PDE inhibitors are sildenafil (a PDE5 inhibitor) and milrinone (a PDE3 inhibitor), each targeting specific pathways to achieve their therapeutic effects. Understanding their mechanisms and applications is essential for optimizing their use in clinical settings.
From an analytical perspective, PDE5 inhibitors like sildenafil and tadalafil are widely recognized for their role in treating erectile dysfunction, but their impact on systemic and coronary vasculature is equally significant. By inhibiting PDE5, these drugs increase cGMP levels, promoting nitric oxide (NO)-mediated smooth muscle relaxation. This mechanism is particularly beneficial in conditions such as pulmonary arterial hypertension (PAH), where sildenafil is used at doses of 20–60 mg three times daily to improve exercise capacity and reduce symptoms. However, their use in coronary vasculature is limited due to potential interactions with nitrates, which can cause severe hypotension. Clinicians must carefully weigh the benefits against risks, especially in patients with cardiovascular comorbidities.
In contrast, PDE3 inhibitors like milrinone and amrinone act on both cAMP and cGMP pathways, providing potent vasodilatory and inotropic effects. These drugs are primarily used in acute heart failure to improve cardiac output and reduce pulmonary capillary wedge pressure. Milrinone, administered intravenously at a loading dose of 50 mcg/kg followed by 0.375–0.75 mcg/kg/min, is particularly effective in patients with refractory heart failure. However, their use is associated with arrhythmias and hypotension, necessitating close monitoring. This comparative analysis highlights the distinct profiles of PDE3 and PDE5 inhibitors, emphasizing the importance of selecting the appropriate agent based on the patient’s condition and risk factors.
A persuasive argument for the broader use of PDE inhibitors lies in their potential to address unmet needs in vascular and cardiac disorders. For instance, emerging research suggests that PDE9 inhibitors, which target cGMP degradation in the heart and vasculature, may offer novel therapeutic options for heart failure and hypertension. Additionally, combination therapies involving PDE inhibitors and other vasodilators could enhance efficacy while minimizing side effects. However, this approach requires rigorous clinical trials to establish safety and efficacy. By advocating for continued research and development, healthcare providers can unlock new applications for these versatile drugs, improving outcomes for patients with vascular and cardiac diseases.
Practically, incorporating PDE inhibitors into treatment regimens requires careful consideration of patient-specific factors. For older adults, dosage adjustments are often necessary due to age-related changes in renal function and drug metabolism. For example, tadalafil doses above 20 mg should be avoided in patients over 65 or those with hepatic impairment. Patients should also be educated about potential side effects, such as headaches, flushing, and dyspepsia, and advised to avoid concomitant use of nitrates. Finally, regular monitoring of blood pressure and cardiac function is essential to ensure safe and effective therapy. These practical tips can help clinicians maximize the benefits of PDE inhibitors while minimizing risks.
Muscle Relaxer Duration: How Long Until Effects Wear Off?
You may want to see also
Frequently asked questions
Nitroglycerin is a commonly used drug that relaxes smooth muscle in both coronary and systemic vasculature by releasing nitric oxide, which activates guanylate cyclase and increases cyclic GMP, leading to vasodilation.
Nitroglycerin works by metabolizing into nitric oxide (NO), which stimulates the production of cyclic guanosine monophosphate (cGMP). This causes relaxation of smooth muscle cells in the vessel walls, resulting in vasodilation of both coronary and systemic arteries.
Yes, other drugs like hydralazine and calcium channel blockers (e.g., nifedipine) also relax smooth muscle in vasculature. Hydralazine acts by directly relaxing arterial smooth muscle, while calcium channel blockers reduce calcium influx, leading to vasodilation in both coronary and systemic vessels.