Muscle inflammation, or myositis, can be caused by a variety of factors, including injury, infection, or illness. Certain medications can also cause drug-induced myopathy, or muscle inflammation. These include statins, fibrates, and fluoroquinolone antibiotics. For example, simvastatin and atorvastatin are statins that can cause muscle inflammation and pain. Additionally, cholesterol-lowering drugs, such as statins, can lead to severe muscle inflammation and damage, affecting muscles throughout the body and even, in rare cases, the heart muscle. Other medications that may cause muscle weakness or pain include antiepileptic drugs, antiarrhythmic medicines, corticosteroids, and isotretinoin. It is important to note that not all individuals who take these medications will develop myopathy, and the benefits and risks should be discussed with a doctor.
| Characteristics | Values |
|---|---|
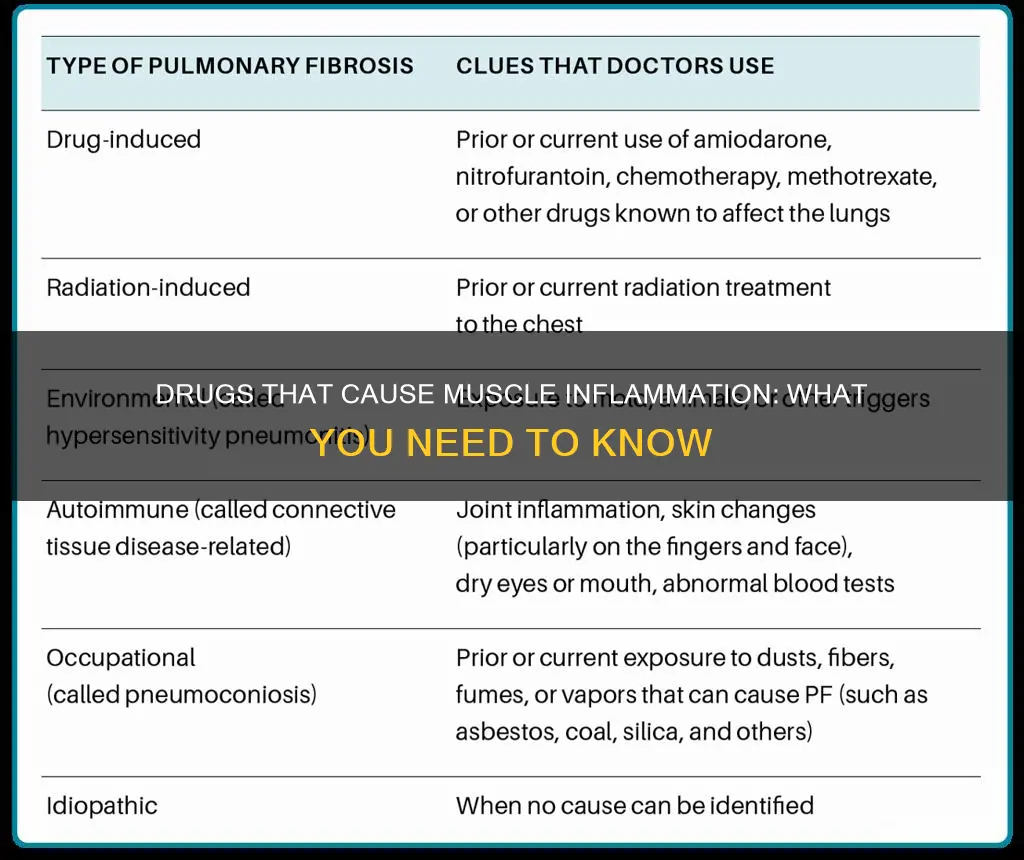
| Drug Types | Statins, Fluoroquinolone antibiotics, Fibrates, Aromatase inhibitors, Oral steroids, Antiepileptic drugs, Omeprazole, Pregabalin, Bisphosphonates |
| Drug Names | Simvastatin, Levofloxacin, Gemfibrozil, Anastrozole, Prednisone, Lamotrigine, Phenytoin, Isotretinoin, Zidovudine |
| Symptoms | Muscle pain, Muscle weakness, Muscle inflammation, Muscle stiffness, Muscle spasms, Muscle cramps |
| Risk Factors | High doses, Prolonged use, Combination with other drugs, Age, Gender |
| Treatment | Lower dosage, Alternative medications, Hot or cold compresses, Over-the-counter pain relievers, Topical treatments |
Explore related products






What You'll Learn
![]()
Statins, fibrates, and antiretroviral drugs
Statins are among the most widely prescribed medications globally, used by over 200 million people to lower cholesterol and their risk of cardiovascular disease. However, statin usage can present certain side effects, the most common of which is myopathy, a painful clinical disorder of the skeletal muscles. This is known as statin-induced myopathy and is experienced by up to a third of statin users. While the mechanism behind statin-induced myopathy is not fully understood, some theories suggest that statins interfere with a protein integral to muscle health and growth, or that they cause a reduction in coenzyme Q10, which is necessary for optimal muscle function. In rare cases, statins can also cause rhabdomyolysis, a life-threatening form of myopathy caused by muscle breakdown and significant creatine kinase elevations.
Fibrates are a class of amphipathic carboxylic acids and esters that are used to treat a range of metabolic disorders, primarily hypercholesterolemia (high cholesterol). They are often used as accessory therapy in many forms of hypercholesterolemia and can reduce the number of non-fatal heart attacks. While fibrates are generally well-tolerated, causing at most mild stomach upset, they can also lead to myopathy. When combined with statin drugs, fibrates can cause a significantly greater reduction in LDL-C and triglyceride levels, increasing the risk of rhabdomyolysis.
Antiretroviral drugs are used in the treatment of HIV and its associated neuromuscular disorders, which can occur at all stages of the disease and affect the peripheral nervous system. Certain antiretrovirals, such as zidovudine (AZT) and stavudine (d4T), may lead to toxic myopathy through impairment of mitochondrial function. Stavudine, didanosine (ddI), and zalcitabine (ddC) are also associated with toxic neuropathy, although they are now less commonly used in resource-rich environments.
Iron Deficiency: The Link to Muscle Pain and Weakness
You may want to see also
Explore related products






![]()
Oral corticosteroids and steroid-induced myopathy
Corticosteroids are a broad group of medications that relieve inflammation, swelling, and pain. They are commonly referred to as "steroids". While they are effective in treating these symptoms, they can also cause several side effects, especially when used long-term. One such side effect is steroid-induced myopathy, a toxic non-inflammatory muscle disease caused by exogenous or endogenous corticosteroid administration.
Steroid-induced myopathy typically affects the pelvic muscles and presents as muscle weakness without pain. It is more common with higher doses of oral or intravenous steroids, although inhaled steroids can also cause muscle weakness in rare cases. The chronic form of the disease occurs after prolonged use of corticosteroids and has an insidious course, while the acute form is less common and occurs abruptly while the patient is receiving high doses of corticosteroids. In both forms, muscle weakness is a common symptom. Case studies have shown that up to 20% of patients exhibit objective signs of muscle weakness, while a subjective feeling of weakness occurs in 60% of patients.
The risk factors for developing steroid-induced myopathy include being female, older age, and a sedentary lifestyle. Women are twice as likely as men to develop muscle weakness from steroid use, although the reason is unclear. Older people are also more susceptible to this condition. Additionally, a sedentary lifestyle may increase the risk of muscle weakness in patients taking corticosteroids, as they seem to affect less active muscles preferentially.
The treatment for steroid-induced myopathy involves reducing or discontinuing the corticosteroid dose, which typically leads to a resolution of the muscle weakness. However, recovery can take weeks or months. Physical therapy, including resistance and aerobic exercise, has also been shown to be beneficial in preventing and treating this condition. In some cases, corticosteroid withdrawal may be necessary to avoid the morbidity associated with the disease.
It is important to note that steroid myopathy may also occur after a short period of oral corticosteroid use. Therefore, if you experience muscle weakness while taking steroids, it is essential to consult your healthcare provider. They may recommend adjusting the dosage, switching to a different medication, or prescribing physical therapy to address the muscle weakness.
Blood Thinners and Muscle Cramps: What's the Link?
You may want to see also
Explore related products






![]()
Fluoroquinolone antibiotics and statins causing joint pain
Fluoroquinolone antibiotics are a group of antibiotics that can cause joint pain. Fluoroquinolones have been linked to a wide range of gastrointestinal symptoms and functional gastrointestinal disorders. They have also been associated with tendon injuries and ligament damage, particularly affecting the Achilles tendon. In a 2001 study, 76% of patients who developed fluoroquinolone-associated tendon disorders experienced tendinitis, and 24% suffered a tendon rupture. Pain is the most common symptom, and it can persist for months after discontinuing the medication.
Fluoroquinolone antibiotics have also been linked to musculoskeletal complications, ranging from mild myalgias to life-threatening rhabdomyolysis. Myalgias are proposed to be the most common adverse effect of fluoroquinolone use, with symptoms typically manifesting within a week of starting treatment. Statins may increase the risk of fluoroquinolone-associated myopathy.
Statins are a class of cholesterol-lowering drugs that can cause muscle pain and inflammation. They have been associated with three types of muscle conditions: muscle aching, which usually resolves within weeks of discontinuing the drug; muscle pain and mild inflammation that may be accompanied by weakness; and severe muscle inflammation and damage, which can affect the entire body, including the heart. The risk of muscle injury is higher when statins are combined with other drugs that can cause muscle damage.
Some of the specific statin drugs that have been linked to muscle pain and inflammation include simvastatin (Zocor), lovastatin (Mevacor), pravastatin (Pravachol), fluvastatin (Lescol), atorvastatin (Lipitor), and cerivastatin (Baycol).
In summary, both fluoroquinolone antibiotics and statins have been associated with joint and muscle pain, with statins also causing muscle inflammation and, in rare cases, severe muscle damage. If you suspect that a medication is causing joint or muscle pain, it is important to consult your healthcare provider for advice and potential alternative treatments.
Muscle Spasms and Peripheral Neuropathy: What's the Link?
You may want to see also
Explore related products






![]()
Selective serotonin reuptake inhibitors (SSRIs) and headaches
Selective serotonin reuptake inhibitors (SSRIs) are a class of drugs typically used as antidepressants to treat major depressive disorder, anxiety disorders, and other psychiatric disorders. They work by blocking serotonin reabsorption (reuptake) via the serotonin transporter, leading to increased serotonin activity and gradual changes in brain signaling and receptor regulation. Serotonin is often referred to as the "feel-good hormone," and it contributes to well-being, mood, appetite, and the regulation of the body's sleep-wake cycle.
SSRIs have been studied for their potential in preventing migraine and tension-type headaches. Migraine is a common neurological disorder that can significantly impair an individual's quality of life. Preventive medications taken before a migraine attack can be beneficial, and due to the role of serotonin in pain mechanisms, SSRIs and serotonin-norepinephrine reuptake inhibitors (SNRIs) have been evaluated for migraine prevention. However, evidence supporting the use of SSRIs for migraine prevention is limited.
One study compared escitalopram, an SSRI, to venlafaxine, a serotonin and weak nor-adrenaline reuptake inhibitor, in patients with migraine without depression or anxiety. The study found that both drugs had similar efficacy in reducing migraine frequency and duration, but escitalopram had a better safety profile. While SSRIs have been shown to increase serotonin levels, excessive levels can lead to serotonin syndrome, causing symptoms such as agitation, confusion, sweating, tremors, and a rapid heart rate.
It is important to note that SSRIs can have side effects, and abrupt discontinuation can lead to withdrawal symptoms such as headache, nausea, vomiting, dizziness, chills, body aches, paresthesias, insomnia, and "brain zaps." SSRIs may also interact with other medications, especially opioids, and can increase the risk of bleeding when taken with certain drugs. Therefore, it is crucial to consult a healthcare professional before starting or discontinuing SSRIs and to gradually taper off the medication to minimize withdrawal symptoms.
How Tension and Muscle Aches Are Linked
You may want to see also
Explore related products






![]()
Opioids and withdrawal symptoms
While searching for drugs that cause muscle inflammation, I found that drug-induced myopathy or muscle disease is a common side effect of certain medications. These include cholesterol-lowering drugs, fibrates, antiarrhythmic medicines, antiepileptic drugs, and oral steroids.
Now, focusing on opioids and withdrawal symptoms:
Opioids are a group of drugs used to manage severe pain and are also commonly misused as psychoactive substances. They include morphine, heroin, oxycontin, codeine, methadone, and hydromorphone hydrochloride. Opioid withdrawal occurs when a patient who is dependent on opioids suddenly reduces or stops taking them. Withdrawal can also be triggered when an opioid is in a patient's system, and they are given an opioid partial agonist or antagonist. Opioid withdrawal is not life-threatening, but it can be very uncomfortable and dangerous to undergo without medical supervision. Symptoms can include rhinorrhea, piloerection, myalgia, diarrhea, nausea/vomiting, pupillary dilation, photophobia, insomnia, autonomic hyperactivity, and yawning. The severity of withdrawal can vary, and pharmacological management is often needed.
Long-term opioid replacement and maintenance medications such as methadone and buprenorphine are commonly used to manage withdrawal. These medications are typically given in inpatient or outpatient treatment settings or detox facilities. Additionally, naltrexone can help prevent relapse and is available in pill or injection form. However, if taken while opioids are still in the system, it can cause sudden and severe withdrawal. Detoxification and withdrawal from opioids can be challenging and should be done very slowly with medical supervision. Treatment often involves medications, counseling, and support, and patients should be checked for depression and other mental illnesses to reduce the risk of relapse. Antidepressants may be prescribed as needed.
If you or someone you know is experiencing opioid withdrawal, it is important to seek professional help. Services such as the National Helpline for Mental Health, Drug, and Alcohol Issues offer free and confidential support 24/7.
Muscle Knots: Do They Cause Inflammation?
You may want to see also
Frequently asked questions
Statins, fibrates, fluoroquinolone antibiotics, and corticosteroids can cause muscle inflammation.
Statins are a group of drugs used to lower cholesterol. They are the most common culprits of muscle inflammation and pain. Examples of statins include lovastatin, simvastatin, pravastatin, fluvastatin, atorvastatin, and cerivastatin.
Fibrates are drugs used to lower cholesterol and triglycerides. Examples of fibrates include gemfibrozil and fenofibrate.
Fluoroquinolone antibiotics are a group of antibiotics that include levofloxacin.
Corticosteroids, also known as steroids, are a group of drugs used to relieve swelling, pain, and inflammation. Examples of corticosteroids include prednisone and dexamethasone.
Note: If you are experiencing muscle inflammation or pain, please consult a medical professional.