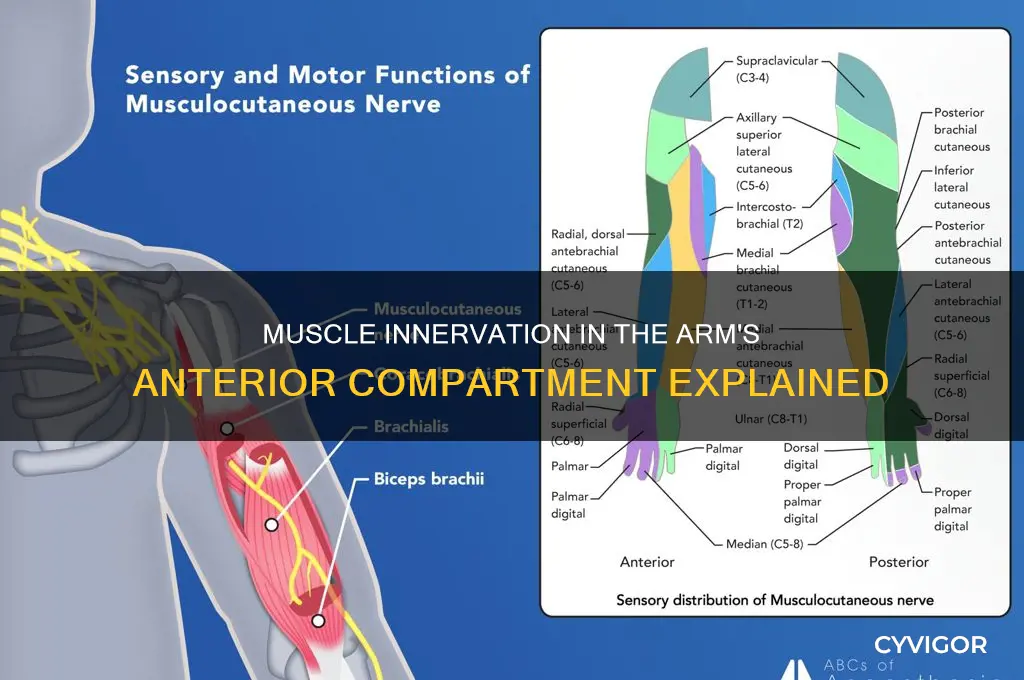
The anterior compartment of the arm is primarily innervated by the musculocutaneous nerve, a branch of the brachial plexus. This nerve supplies motor innervation to the muscles within this compartment, which include the biceps brachii, responsible for elbow flexion and forearm supination, the brachialis, assisting in elbow flexion, and the coracobrachialis, involved in shoulder adduction and flexion. The musculocutaneous nerve ensures coordinated movement and strength in these muscles, playing a crucial role in upper limb function. Additionally, it provides sensory innervation to the lateral aspect of the forearm, further highlighting its importance in both motor and sensory pathways. Understanding the innervation of the anterior arm compartment is essential for diagnosing and treating conditions affecting these muscles and nerves.
| Characteristics | Values |
|---|---|
| Nerve | Musculocutaneous nerve (C5-C7) |
| Root Value | C5-C7 |
| Nerve Type | Mixed (motor and sensory) |
| Muscles Innervated | Coracobrachialis, Biceps brachii, Brachialis |
| Action of Innervated Muscles | Flexion of elbow, supination of forearm, adduction of arm |
| Sensory Distribution | Lateral forearm (via lateral antebrachial cutaneous nerve) |
| Origin of Nerve | Lateral cord of brachial plexus |
| Course | Passes between biceps and brachialis, then pierces coracobrachialis |
| Clinical Relevance | Injury can result in weakness in elbow flexion and forearm supination, and sensory loss over lateral forearm |
Explore related products



$21.95 $24.95



What You'll Learn
- Musculocutaneous Nerve: Innervates coracobrachialis, biceps brachii, brachialis muscles in anterior arm compartment
- Nerve Roots: Originates from C5-C7 cervical nerve roots, supplying anterior compartment muscles
- Nerve Pathway: Travels through coracobrachialis, then between biceps and brachialis muscles
- Muscle Actions: Enables flexion, supination, and stabilization of the arm and forearm
- Clinical Relevance: Damage causes weakness in elbow flexion and forearm supination
![]()
Musculocutaneous Nerve: Innervates coracobrachialis, biceps brachii, brachialis muscles in anterior arm compartment
The musculocutaneous nerve is a critical player in the function of the anterior compartment of the arm, specifically innervating the coracobrachialis, biceps brachii, and brachialis muscles. This nerve, a branch of the lateral cord of the brachial plexus, originates from the cervical spine's C5-C7 nerve roots. Its role is essential for movements such as flexion of the elbow and shoulder, highlighting its importance in everyday activities like lifting objects or reaching overhead. Understanding the musculocutaneous nerve's function is key for healthcare professionals diagnosing nerve injuries or planning surgical interventions in the upper limb.
Consider the practical implications of musculocutaneous nerve damage. A common injury, often resulting from shoulder dislocations or compression, can lead to weakness in elbow flexion and a diminished biceps reflex. Patients may report difficulty in tasks requiring arm strength, such as carrying groceries or performing push-ups. Clinicians assess this nerve's integrity through specific tests, including the biceps reflex hammer test and manual muscle testing of the innervated muscles. Early detection and targeted rehabilitation, including nerve gliding exercises and progressive resistance training, can significantly improve recovery outcomes.
From an anatomical perspective, the musculocutaneous nerve's pathway is both precise and vulnerable. It courses through the arm, piercing the coracobrachialis muscle before continuing as the lateral cutaneous nerve of the forearm. This route makes it susceptible to compression at several points, particularly at the shoulder and elbow. For instance, repetitive motions or prolonged pressure in these areas can lead to conditions like neuropraxia, a temporary nerve dysfunction. Awareness of this anatomy is crucial for athletes, manual laborers, and anyone at risk of nerve compression, as preventive measures such as ergonomic adjustments and stretching can mitigate potential issues.
In clinical settings, differentiating musculocutaneous nerve injuries from other pathologies is vital. For example, symptoms like forearm numbness or weakness might overlap with radial or median nerve issues. Electromyography (EMG) and nerve conduction studies (NCS) are invaluable tools for accurate diagnosis, pinpointing the exact location and severity of nerve damage. Treatment options range from conservative management, including physical therapy and anti-inflammatory medications, to surgical decompression in severe cases. Patient education on activity modification and the importance of gradual return to function is equally important for long-term recovery.
Finally, the musculocutaneous nerve's role extends beyond mere muscle innervation; it also contributes to sensory function in the lateral forearm via its terminal branch. This dual responsibility underscores its significance in both motor and sensory pathways. For individuals experiencing symptoms, a comprehensive approach addressing both strength and sensation is essential. Incorporating sensory re-education techniques, such as texture discrimination exercises, alongside traditional strength training can enhance overall functional recovery. By focusing on this nerve's unique attributes, healthcare providers can offer more tailored and effective care for patients with anterior arm compartment issues.
Sculpted Arms Year-Round: Achieve and Maintain Muscle Definition Easily
You may want to see also
Explore related products






![]()
Nerve Roots: Originates from C5-C7 cervical nerve roots, supplying anterior compartment muscles
The muscles in the anterior compartment of the arm, primarily the biceps brachii and brachialis, are innervated by the musculocutaneous nerve. This nerve originates from the cervical nerve roots C5-C7, a critical detail for understanding both anatomy and potential clinical implications. These roots combine to form the lateral cord of the brachial plexus, from which the musculocutaneous nerve arises. This pathway ensures precise motor control of elbow flexion and forearm supination, essential for activities ranging from lifting objects to turning doorknobs.
Analyzing the role of C5-C7 roots reveals their significance in upper limb function. Damage to these roots, often due to trauma or compression (e.g., cervical disc herniation), can result in weakened or paralyzed biceps and brachialis muscles. Clinicians assess C5-C7 integrity by testing biceps reflex and strength, with abnormalities indicating potential nerve root pathology. For instance, a diminished biceps reflex may suggest C5 or C6 root involvement, guiding diagnostic imaging or further neurological evaluation.
From a practical standpoint, understanding this innervation is vital for targeted rehabilitation. Patients with C5-C7 root injuries benefit from exercises focusing on elbow flexion and forearm supination, such as biceps curls or resistance band supination exercises. Early intervention, including nerve gliding techniques and gradual strengthening, can improve recovery outcomes. For older adults or those with chronic conditions, low-resistance exercises (e.g., 1-2 kg weights) are recommended to avoid strain while promoting muscle activation.
Comparatively, the posterior compartment muscles (e.g., triceps) are innervated by the radial nerve, which originates from different cervical roots (C6-C8). This distinction highlights the specificity of nerve root contributions to arm function. While radial nerve injuries affect elbow extension, musculocutaneous nerve damage impacts flexion, underscoring the need for precise anatomical knowledge in diagnosis and treatment.
In conclusion, the C5-C7 cervical nerve roots play a pivotal role in innervating the anterior compartment muscles of the arm via the musculocutaneous nerve. This knowledge is essential for clinicians, therapists, and patients alike, enabling accurate assessment, targeted rehabilitation, and improved functional outcomes. Whether addressing acute injuries or chronic conditions, focusing on these nerve roots ensures a comprehensive approach to upper limb health.
Understanding the Major Arm Muscles: A Comprehensive Guide
You may want to see also
Explore related products






![]()
Nerve Pathway: Travels through coracobrachialis, then between biceps and brachialis muscles
The musculocutaneous nerve is a key player in the innervation of the anterior compartment of the arm, following a distinct pathway that ensures precise muscle control. Originating as a branch of the brachial plexus, it embarks on a journey through the coracobrachialis muscle, a small but significant structure that assists in arm adduction and stabilization. This initial passage is crucial, as it sets the stage for the nerve’s subsequent role in powering the primary movers of the arm.
After traversing the coracobrachialis, the musculocutaneous nerve continues its course, strategically positioned between the biceps brachii and brachialis muscles. This anatomical arrangement is not arbitrary; it allows the nerve to efficiently innervate both muscles, which are essential for elbow flexion. The biceps brachii, often associated with strength and aesthetics, relies on this nerve supply to contract and shorten, pulling the forearm toward the upper arm. Simultaneously, the brachialis, a deeper muscle, contributes to the same movement, ensuring smooth and powerful flexion.
Understanding this pathway is vital for clinicians and anatomists alike, as it informs diagnostic and therapeutic approaches. For instance, damage to the musculocutaneous nerve in this region can result in weakened elbow flexion and a loss of sensation in the lateral forearm. Practitioners can localize injuries more accurately by tracing the nerve’s route, from its passage through the coracobrachialis to its distribution between the biceps and brachialis. This knowledge also aids in surgical planning, ensuring that procedures avoid compromising nerve integrity.
For fitness enthusiasts and athletes, awareness of this nerve pathway underscores the importance of balanced training. Overemphasis on the biceps without considering the brachialis or coracobrachialis can lead to muscle imbalances and increased injury risk. Incorporating exercises that target all three muscles—such as hammer curls for the brachialis and static arm holds for the coracobrachialis—ensures comprehensive development and nerve health. Practical tips include maintaining proper form during weightlifting and integrating stretching routines to alleviate nerve compression.
In summary, the musculocutaneous nerve’s journey through the coracobrachialis and between the biceps and brachialis muscles is a masterclass in anatomical efficiency. This pathway not only facilitates essential arm movements but also highlights the interconnectedness of muscles and nerves. Whether for medical diagnosis, surgical precision, or fitness optimization, understanding this route provides actionable insights that translate into better outcomes.
Effective Remedies to Relieve Swollen Arm Muscles Fast and Safely
You may want to see also
Explore related products






![]()
Muscle Actions: Enables flexion, supination, and stabilization of the arm and forearm
The anterior compartment of the arm is a powerhouse of movement, housing muscles that work in harmony to enable essential actions like flexion, supination, and stabilization. At the heart of this coordination lies the musculocutaneous nerve, which innervates the primary muscles responsible for these functions: the biceps brachii, coracobrachialis, and brachialis. Understanding how these muscles interact and the nerve that drives them is key to appreciating the arm’s functional anatomy.
Consider the biceps brachii, the most prominent muscle in this compartment. Its dual role in flexion and supination is a testament to its anatomical design. When you lift a dumbbell or turn a doorknob, the biceps contracts, pulling the forearm toward the shoulder (flexion) while simultaneously rotating the palm upward (supination). This action is made possible by the musculocutaneous nerve’s precise signaling, ensuring synchronized muscle activation. For optimal strength training, incorporate exercises like hammer curls (for brachioradialis engagement) and traditional bicep curls (for biceps brachii), aiming for 3 sets of 8–12 repetitions, 2–3 times weekly.
Stabilization, often overlooked, is equally critical. The coracobrachialis and brachialis contribute to forearm stability during dynamic movements, preventing unwanted wobbling or strain. For instance, during a bench press, these muscles stabilize the arm while the triceps extend the elbow. To enhance stabilization, integrate isometric holds—such as holding a dumbbell halfway through a curl—for 10–15 seconds, repeated 3–4 times per session. This builds endurance in the anterior compartment muscles, reducing injury risk.
A comparative analysis reveals the musculocutaneous nerve’s efficiency in distributing motor signals. Unlike the radial or median nerves, which innervate posterior or lateral muscles, the musculocutaneous nerve focuses solely on the anterior compartment, ensuring specialized control. This division of labor allows for precise, isolated movements, such as supination without concurrent flexion. For rehabilitation or injury prevention, focus on nerve gliding exercises: gently rotate the forearm in circles, alternating directions, for 1 minute daily to maintain nerve mobility.
In practical terms, understanding this innervation helps diagnose and treat conditions like musculocutaneous nerve entrapment, which can cause weakness in flexion and supination. If you experience persistent forearm pain or reduced grip strength, consult a physical therapist for targeted exercises. For athletes, balancing strength training with flexibility work—like wrist stretches—ensures the anterior compartment functions optimally. By prioritizing both power and precision, you unlock the full potential of these muscles, whether in daily activities or high-performance sports.
Why Your Arm Muscle is Twitching: Causes and Solutions Explained
You may want to see also
Explore related products




![]()
Clinical Relevance: Damage causes weakness in elbow flexion and forearm supination
The muscles in the anterior compartment of the arm, primarily the biceps brachii and brachialis, are innervated by the musculocutaneous nerve, a branch of the brachial plexus. This nerve plays a critical role in transmitting signals that enable elbow flexion and forearm supination. When damage occurs to the musculocutaneous nerve, the clinical consequences are immediate and functionally significant, manifesting as weakness in these specific movements. Understanding this relationship is essential for diagnosing and managing conditions that affect upper limb function.
Consider a patient presenting with difficulty lifting objects or turning their palm upward—classic signs of weakened elbow flexion and forearm supination. Clinically, this could stem from musculocutaneous nerve injury, often caused by compression (e.g., from a tight cast or prolonged pressure), trauma, or surgical complications. For instance, a 45-year-old construction worker with a history of repetitive arm movements might develop nerve compression over time, leading to gradual onset weakness. In contrast, a 25-year-old athlete could experience acute trauma during a fall, resulting in immediate loss of function. Early recognition of these symptoms is crucial, as delayed intervention can lead to irreversible muscle atrophy and functional decline.
Diagnosis typically involves a combination of clinical examination and electrophysiological studies. During the exam, the clinician may observe reduced biceps reflex and test specific muscle strength using a 0-to-5 manual muscle testing scale. Electromyography (EMG) and nerve conduction studies (NCS) can confirm the location and severity of the nerve damage. For mild cases, conservative management—including physical therapy, anti-inflammatory medications, and activity modification—may suffice. Severe cases, however, might require surgical decompression or nerve repair, particularly if symptoms persist beyond 6 months or if there is evidence of significant axonal loss.
Rehabilitation focuses on restoring strength and function through targeted exercises. Patients should start with gentle range-of-motion exercises, progressing to resistance training as tolerated. Practical tips include using resistance bands for biceps curls and forearm pronation/supination exercises with light weights. It’s important to avoid overloading the muscles during recovery, as this can exacerbate the injury. For older adults or those with comorbidities, a gradual, supervised program is recommended to minimize the risk of further damage.
In summary, damage to the musculocutaneous nerve directly impacts elbow flexion and forearm supination, with clinical implications ranging from mild weakness to severe functional impairment. Prompt diagnosis, tailored treatment, and structured rehabilitation are key to optimizing outcomes. By understanding the specific role of this nerve in upper limb function, healthcare providers can effectively address the unique challenges posed by such injuries.
Understanding the Upper Arm Muscle: Biceps and Triceps Explained
You may want to see also
Frequently asked questions
The musculocutaneous nerve primarily innervates the muscles in the anterior compartment of the arm.
The musculocutaneous nerve innervates the coracobrachialis, biceps brachii, and brachialis muscles in the anterior compartment of the arm.
No, the radial nerve primarily innervates the muscles in the posterior and lateral compartments of the arm, not the anterior compartment.
The musculocutaneous nerve originates from the lateral cord of the brachial plexus and passes through the coracobrachialis muscle to innervate the anterior compartment of the arm.