Muscle atonia is a condition characterised by a sustained loss of normal muscle function during REM sleep. It is one of the defining features of REM sleep, and its presence or absence can have significant implications for our understanding and treatment of various sleep disorders. The study of muscle atonia during sleep is important in revealing the underlying mechanisms of sleep disorders, such as REM behaviour disorder, narcolepsy, and cataplexy. The condition is also associated with increased muscle tone during sleep, allowing for the physical acting out of dreams, which can sometimes result in injury.
Explore related products

$35.6 $43.95





What You'll Learn
- REM sleep is characterised by fast, desynchronised rhythms in the EEG, hippocampal theta activity, and rapid eye movements
- Motoneurons are not generating action potentials during REM sleep
- REM sleep behaviour disorder (RBD) is a parasomnia where patients act out their dreams, sometimes resulting in injury
- Cataplexy, which affects people with narcolepsy, is characterised by a bilateral loss of muscle tone while awake
- The brain circuitry governing REM sleep is located in the pontine and medullary brainstem
![]()
REM sleep is characterised by fast, desynchronised rhythms in the EEG, hippocampal theta activity, and rapid eye movements
Rapid eye movement (REM) sleep is a unique sleep phase characterised by fast, desynchronised rhythms in the EEG, hippocampal theta activity, and rapid eye movements. This phase is associated with vivid dreams and occurs in all land mammals and birds.
REM sleep is characterised by high levels of acetylcholine in the hippocampus, which suppress feedback from the hippocampus to the neocortex. In contrast, lower levels of acetylcholine and norepinephrine in the neocortex allow the uncontrolled spread of associational activity within neocortical areas. This process is thought to add creativity by allowing "neocortical structures to reorganise associative hierarchies, in which information from the hippocampus would be reinterpreted in relation to previous semantic representations or nodes".
The electrical and chemical activity regulating this sleep phase originates in the brain stem and is characterised by an abundance of the neurotransmitter acetylcholine and a near absence of monoamine neurotransmitters such as histamine, serotonin, and norepinephrine. The high levels of acetylcholine in the hippocampus during REM sleep result in theta oscillations, which are also observed during waking exploration.
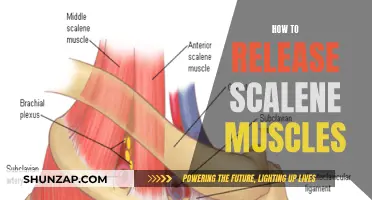
During REM sleep, muscle atonia occurs when motoneurons are not generating action potentials. This loss of muscle tone during REM sleep is one of its defining features and is mediated by a highly specialised neuronal system. The supraspinal mechanisms responsible for REM atonia originate in the perilocus coeruleus (LC)-alpha nucleus in the pons, which sends excitatory projections to the nucleus reticularis magnocellularis in the medulla. This results in muscle atonia, preventing the physical acting out of dreams.
However, in some cases, REM behaviour disorder can cause increased muscle tone during REM sleep, allowing movement and the acting out of dreams, which can result in physical injury.
The Sphincter Muscle's Role and Importance in Human Health
You may want to see also
Explore related products






![]()
Motoneurons are not generating action potentials during REM sleep
Muscle atonia is a fundamental characteristic of REM sleep. It is defined by the sustained (tonic) loss of normal muscle atonia during REM sleep. This loss of muscle tone is due to the inhibition of motoneurons, which are not generating action potentials.
During the tonic periods of REM sleep, motoneurons do not generate action potentials. Motoneuron action potentials arise at the initial segment of the cell's axon, close to its soma, and result from a summation of currents generated at synapses on the soma and dendrites. If the voltage produced by these currents is above a certain threshold, an action potential is triggered.
Research has focused on three processes as likely contributors to the decreased discharge of motoneurons during REM sleep: postsynaptic inhibition, disfacilitation (or withdrawal of excitatory input), and presynaptic inhibition of muscle afferents. Some combination of these three processes is also possible.
Intracellular recordings from motoneurons during sleep and wakefulness have been used to determine the basis for atonia during REM sleep. These recordings have identified mechanisms responsible for the suppression of motoneuron excitability during REM sleep.
The neurotransmitters responsible for the inhibition of motoneurons during REM sleep have also been studied. For example, strychnine (a glycine receptor antagonist) and bicuculline (a GABAA receptor antagonist) have been microiontophoretically applied adjacent to the cell body of motoneurons while recording intracellularly during sleep and wakefulness.
Myoglobin and Muscles: What's the Rich Connection?
You may want to see also
Explore related products





![]()
REM sleep behaviour disorder (RBD) is a parasomnia where patients act out their dreams, sometimes resulting in injury
Muscle atonia is a state of sustained loss of normal muscle tone during REM sleep. It is mediated by an active and highly specialised neuronal system. During the tonic periods of REM sleep, motoneurons do not generate action potentials, resulting in muscle atonia.
The diagnosis of RBD is suggested by a careful evaluation but should be confirmed by a sleep study to evaluate abnormal muscle tone during REM sleep and rule out other sleep disorders. A sleep history may help identify whether the symptoms are occurring during the REM or non-REM stage of sleep. A video-monitored polysomnographic study is often used to distinguish RBD from other sleep disorders.
Treatment for RBD focuses on creating a safe sleeping environment to prevent injuries. Medications such as melatonin, clonazepam, and pramipexole have been shown to reduce symptoms in some cases, although there are currently no FDA-approved medications specifically for RBD.
Carbs: Fueling Muscles and Performance
You may want to see also
Explore related products





![]()
Cataplexy, which affects people with narcolepsy, is characterised by a bilateral loss of muscle tone while awake
Muscle atonia is a sustained (tonic) loss of normal muscle activity during REM sleep. It is mediated by an active and highly specialised neuronal system. During muscle atonia, motoneurons do not generate action potentials.
Cataplexy is a symptom of narcolepsy, a sleep disorder characterised by excessive daytime sleepiness, sleep paralysis, hallucinations, and, in some cases, cataplexy. Cataplexy is characterised by a bilateral loss of muscle tone while awake. It is differentiated from other conditions that cause a loss of muscle control, such as fainting or seizures, by the fact that people experiencing cataplexy remain conscious and aware. Cataplexy can be triggered by strong emotions, especially positive emotions like laughter, witty conversations, and pleasant surprises. However, it can also be triggered by anger, fear, or excitement. The severity of cataplexy episodes varies, with mild cases affecting only the face and neck, while more severe cases can cause a person to collapse to the ground.
The two main types of narcolepsy are type 1 and type 2. Type 1 narcolepsy, previously known as narcolepsy with cataplexy, is characterised by the presence of cataplexy and excessive daytime sleepiness. It is diagnosed by detecting low levels of hypocretin (also known as orexin), a natural chemical that helps maintain sleep-wake stability and controls REM sleep. Type 2 narcolepsy, previously known as narcolepsy without cataplexy, does not typically involve cataplexy. While the cause of type 1 narcolepsy is well understood (loss of the neurotransmitter orexin), the cause of type 2 narcolepsy is not yet well understood.
Research has shown that people with cataplexy exhibit a loss of certain brain cells that produce the hormone orexin. This loss of orexin is irreversible, but treatments can help decrease the frequency of cataplexy episodes. Orexin-based therapies are being investigated as a potential treatment option for narcolepsy, with the aim of helping people stay awake and manage their symptoms.
Building Strong Ab Muscles: A Guide to Development
You may want to see also
Explore related products






![]()
The brain circuitry governing REM sleep is located in the pontine and medullary brainstem
Muscle atonia refers to the loss of muscle tone during REM sleep, which is a fundamental characteristic of this sleep stage. The brain circuitry governing REM sleep is located in the pontine and medullary brainstem, specifically in the dorsal pontine brainstem. This region is critical for the generation of muscle atonia during REM sleep. Within the brainstem, the peri-locus coeruleus (LC) α region in the pontine tegmentum is crucial for inducing REM sleep. The sublaterodorsal nucleus (SLD) in rodents is homologous to the cat peri-LC-α. Inhibition of glutamatergic neurotransmission in the SLD reduces REM sleep and impairs muscle atonia.
The pontine-medullary loop is essential for REM sleep, and its deficit is associated with Parkinson's disease. Neurons in the pontine sublaterodorsal tegmentum (SubLDT) that express corticotropin-releasing hormone-binding protein (Crhbp+ neurons) project to the medulla and promote REM sleep. Within the medulla, neurons expressing nitric oxide synthase 1 (Nos1+ neurons) project back to the SubLDT, forming a positive interaction between the pons and the medulla. This loop operates as a core REM sleep circuit. Ablating Crhbp+ neurons reduces sleep and impairs REM sleep atonia.
The medulla also plays a crucial role in controlling REM sleep. Specifically, the dorsomedial medulla (dmM) neurons expressing corticotropin-releasing hormone (CRH) regulate REM sleep. These dmM CRH neurons are selectively activated during REM sleep and are considered a hub in the REM sleep circuitry. The dmM CRH neurons also promote enhanced pontine wave density, which is a hallmark of REM sleep.
Damage to the brainstem circuits that produce normal REM sleep can result in REM behaviour disorder (RBD). RBD is characterised by dream-enacting body movements due to dysregulation of muscle atonia during REM sleep. This disorder is often a prodromal marker of synucleinopathies, including Parkinson's disease. Clinical and scientific data indicate that RBD is caused by damage to the brainstem circuits, and it is considered the earliest symptom of these disorders.
Exploring the Intriguing Syllable Count in the Word 'Muscles
You may want to see also
Frequently asked questions
Muscle atonia is the loss of normal muscle tone during rapid eye movement (REM) sleep. It is one of the defining features of REM sleep.
During muscle atonia, motoneurons do not generate action potentials. This results in a complete loss of muscle tone in axial postural muscles, phasic muscle twitches in distal limb and orofacial muscles, and phasic bursting of oculomotor muscles.
The mechanisms causing muscle atonia are complex and not yet fully understood. However, research has focused on three processes as likely contributors: postsynaptic inhibition, disfacilitation, and presynaptic inhibition of muscle afferents.
Muscle atonia is important for understanding and treating sleep-related disorders such as REM sleep behaviour disorder (RBD), narcolepsy, and obstructive sleep apnea. In RBD, the absence of muscle atonia can lead to acting out of dreams, sometimes resulting in physical injury.