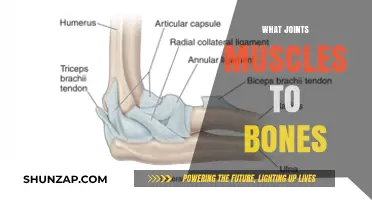
The cardiac muscle, also known as the myocardium, is one of three types of vertebrate muscle tissues, the others being skeletal muscle and smooth muscle. The heart consists mostly of cardiac muscle cells, which are striated, branched, and contain many mitochondria. The length of cardiac muscle in a resting individual is not at its optimal length for contraction. Greater cardiac muscle length, such as occurs with greater ventricular filling, will result in additional stretching of the cardiac muscle, increasing the muscle length and increasing the force of contraction. The force of cardiac muscle contraction can be recorded, with the Y axis showing grams of tension and the X axis showing time in seconds.
| Characteristics | Values |
|---|---|
| Type of Muscle Tissue | Cardiac muscle, also called heart muscle or [myocardium], is one of three types of vertebrate muscle tissues, the others being skeletal muscle and smooth muscle. |
| Contractibility | Cardiac muscle contracts in a similar manner to skeletal muscle. Electrical stimulation triggers the release of calcium from the cell's internal calcium store, the sarcoplasmic reticulum. |
| Diseases | Diseases of the heart muscle are called cardiomyopathies. These include ischemic conditions caused by restricted blood supply to the muscle, such as angina and myocardial infarction. |
| Composition | Myocardial tissue is composed of contractile cardiomyocytes, cardiac fibroblasts, nerve cells, vascular cells, and connective tissue. |
| Length and Contraction | Greater cardiac muscle length results in additional stretching of the muscle, increasing the force of contraction. |
| Contraction Process | During contraction, both the I and A bands lengthen, while neither the H band nor the I band shortens. |
| Control | Cardiac muscle is under involuntary control. |
| Metabolism | Cardiac muscle behaves like skeletal muscle, deriving energy from carbohydrates, ketones, amino acids, and lipids. |
Explore related products






What You'll Learn
![]()
Greater ventricular filling
The primary function of cardiac muscle is to pump blood into circulation by generating sufficient force. The force of contraction of the cardiac muscle is directly proportional to its length. Greater ventricular filling results in increased stretching of the cardiac muscle, which lengthens the muscle and increases the force of contraction. This phenomenon is observed in recordings of electrically stimulated ventricular muscle contractions.
Ventricular filling is a complex process influenced by various factors, including the ventricular myocardial band (VMB), elastic recoil, muscular contraction, and intra-cavitary blood volume (hemoskeleton). The VMB is a structure within the ventricular myocardium that governs electrical, mechanical, and energetical events in the human heart. The specific spatial arrangement and interaction of VMB fibres contribute to the physical principles underlying ventricular filling.
Elastic recoil and muscular contraction are mentioned as mechanisms involved in ventricular suction, but their exact roles remain unclear. Ventricular suction filling is achieved through an increase in ventricular volume and lengthening of its long axis, resulting from ventricular myocardial contraction. This process occurs during the last part of classical systole and the initial third of classical diastole, which includes the isovolumetric relaxation and rapid filling phases.
Diastole, the period of ventricular relaxation and filling, begins with the closing of the aortic valve and ends with the closing of the mitral valve. During diastole, blood vessels return blood to the heart in preparation for the next ventricular contraction. The energy propelling the blood into the ventricle during diastole comes from the potential energy stored in the elasticity of the blood vessels. Ventricular filling is a critical aspect of the cardiac cycle, ensuring the efficient functioning of the heart.
Masseter Muscle: Why is Mine So Big?
You may want to see also
Explore related products






![]()
Electrical stimulation
In terms of electrical stimulation techniques, cardiac muscle experiments often involve the use of isolated strips of toad ventricular muscle that are electrically stimulated to contract. This approach helps researchers study the factors influencing cardiac muscle contraction and its length. Additionally, electrical stimulation is employed in the field of cardiac tissue engineering to stimulate human cell-derived constructs. While these constructs have shown increasing functional maturity, they have not yet reached the functionality of native cardiac tissue.
The application of electrical stimulation in medicine is also noteworthy. For instance, cardiologists may implant artificial pacemakers in patients to regulate heart rate and maintain effective blood pumping. These devices deliver electrical impulses to the heart muscle, ensuring its continuous contraction. Furthermore, electrical muscle stimulation (EMS) has been explored as a training method for patients with stable chronic heart failure. Studies have indicated that prolonged EMS can lead to improvements in strength, peak VO2, and exercise capacity in these patients.
It is important to note that the electrical stimulation of cardiac muscle is a complex process that involves the release of calcium from the sarcoplasmic reticulum, the cell's internal calcium store. This release is triggered by a cardiac action potential, resulting in the contraction of the cardiac muscle. The electrical impulse typically begins at the apex of the heart, causing the contraction to initiate at the apex and travel towards the base.
In conclusion, electrical stimulation is a critical aspect of cardiac muscle function and lengthening. It plays a role in both the intrinsic properties of the cardiac muscle and its therapeutic applications. While significant advancements have been made in understanding and utilizing electrical stimulation, further research is likely ongoing to optimize its potential in various medical contexts, including cardiac tissue engineering and the treatment of cardiac conditions.
Alcohol's Impact on Muscle Inflammation: What's the Truth?
You may want to see also
Explore related products






![]()
Rhythmicity
The cardiac muscle, also known as the myocardium, is one of three types of vertebrate muscle tissues, the others being skeletal muscle and smooth muscle. The myocardium constitutes the main tissue of the heart wall and is responsible for the contractility of the heart, and therefore the pumping action.
Cardiac muscle cells, or cardiomyocytes, are striated, branched, and contain many mitochondria. They are under involuntary control, with their rhythmic contractions regulated by the sinoatrial node of the heart.
The rhythmic contractions of the cardiac muscle are essential for maintaining the pumping action of the heart. These contractions are influenced by the length of the muscle fibres. When the cardiac muscle lengthens, such as during ventricular filling, it results in additional stretching of the muscle fibres. This increased muscle length leads to a stronger contraction, as the force of contraction is directly proportional to the muscle length.
The Frank-Starling law of the heart describes the relationship between muscle length and contraction. It states that during each heartbeat, cardiac muscle cells experience changes in length and load, allowing the heart to adjust its output to meet new physiological and pathological demands.
The spontaneous rhythmic electrical and mechanical activity of cultured myocardial cells is widely studied to understand cardiac physiology. The stimulation of the vagus nerve, for example, increases the permeability of cardiac pacemaker cells to potassium ions, lengthening the repolarisation time and decreasing the rate of heartbeats. This highlights the intricate regulatory mechanisms that influence the rhythmicity of cardiac muscle contractions.
Understanding Psoas Muscle Abscess: Causes, Symptoms, and Treatment
You may want to see also
Explore related products






![]()
Cardiomyopathies
Cardiac muscle, also called heart muscle or myocardium, is one of three types of vertebrate muscle tissues, the others being skeletal muscle and smooth muscle. Cardiomyopathies are diseases of the heart muscle that make it difficult for the heart to pump blood to the rest of the body. Cardiomyopathies weaken the heart muscle, and as the disease worsens, the heart becomes less able to pump blood and maintain a normal electrical rhythm. This can result in heart failure or irregular heartbeats called arrhythmias. A weakened heart can also cause other complications, such as heart valve problems.
There are several types of cardiomyopathies, which differ based on their cause and how they affect the heart's structure and function. Some types are rarer than others, and certain types are temporary and improve over time. Some people may have overlapping cardiomyopathies, such as dilated cardiomyopathy and arrhythmogenic cardiomyopathy. Dilated cardiomyopathy is a common type that occurs when the ventricles, or lower chambers of the heart, become weaker and larger, making it harder for the heart to pump blood efficiently. This can lead to an increased workload for the heart.
Hypertrophic cardiomyopathy is another type of cardiomyopathy where the heart muscle becomes larger and thicker than normal. The thickened areas can block the ventricles, further impeding blood flow. Arrhythmogenic cardiomyopathy is a rare condition that develops when fatty or scarred tissue replaces normal muscle tissue in the right ventricle, leading to an irregular heartbeat. Restrictive cardiomyopathy is also rare and causes the ventricles to stiffen, resulting in reduced blood flow to the rest of the body.
Cardiomyopathy can be acquired when it develops due to another disease, condition, or factor, or it can be inherited when the gene for the disease is passed on from a parent. In many cases, the cause of cardiomyopathy is unknown, especially when it occurs in children. Cardiomyopathy can affect individuals of all ages, although certain age groups are more susceptible to specific types. Some cases of cardiomyopathy may not exhibit any signs or symptoms and may not require treatment. However, in other instances, cardiomyopathy can progress rapidly with severe symptoms and serious complications, necessitating treatment in the form of lifestyle changes, medications, surgery, implanted devices to correct arrhythmias, or other nonsurgical procedures.
The force of cardiac muscle contraction is a crucial factor in cardiomyopathies. Greater ventricular filling leads to increased stretching of the cardiac muscle, resulting in augmented muscle length and a stronger contraction force. However, it is important to note that the length of cardiac muscle in a resting individual is not optimal for contraction.
Muscle Structure: Understanding the Intricate Design of Muscles
You may want to see also
Explore related products





![]()
Sarcomeres
Cardiac muscle, or myocardium, is one of three types of vertebrate muscle tissues, the other two being skeletal muscle and smooth muscle. It is an involuntary, striated muscle that constitutes the main tissue of the heart wall.
Cardiac muscle is made up of sarcomeres, which are the basic contractile units of a myocyte (muscle fibre). Each sarcomere is composed of two main protein filaments: actin and myosin. These filaments are the active structures responsible for muscular contraction.
The widely accepted theory describing muscular contraction is the sliding filament theory. This theory proposes that active force is generated as actin filaments slide past the myosin filaments, resulting in the contraction of an individual sarcomere. During contraction, a sarcomere shortens like a collapsing telescope as the actin filaments at each end of a central myosin filament slide towards the myosin's centre. This movement of myosin appears like a molecular dance, with the myosin reaching forward to bind to the actin, contracting, and then releasing the actin before reaching forward again to bind the actin in a new cycle.
The contraction of the myosin's S1 region is called the power stroke, which requires the hydrolysis of ATP (Adenosine triphosphate). This process breaks a high-energy phosphate bond to release energy, resulting in force generation and the shortening of an individual sarcomere. The simultaneous contraction of sarcomeres, which are joined end-to-end throughout an entire muscle fibre, leads to the shortening of the entire muscle.
Sarcomere lengths are non-uniform on all structural levels of mammalian skeletal muscle. Studies have also shown that in vivo sarcomere lengths become more non-uniform upon activation in intact whole muscle. Additionally, research has been conducted to understand sarcomere length non-uniformities in skeletal muscles.
Running for Muscle Gain: Is It Effective?
You may want to see also
Frequently asked questions
Cardiac muscle, also called myocardium, is one of the three major categories of muscles in the human body, alongside smooth muscle and skeletal muscle. It is involuntary and striated, constituting the main tissue of the heart wall.
During each heartbeat, cardiac muscle cells experience changes in length and load, following the Frank-Starling law of the heart. Greater ventricular filling leads to increased stretching of the cardiac muscle, resulting in greater muscle length and contraction force.
Cardiac output refers to the amount of blood pumped by the heart per minute, which varies based on the body's metabolic needs. Longer cardiac muscles, by virtue of their increased contraction force, can enhance cardiac output to meet these demands.
Yes, the stimulation of the vagus nerve can lengthen the repolarisation time of cardiac pacemaker cells, reducing the heart rate and, consequently, the rate of cardiac muscle contractions.