Eye adduction, the movement of the eye inward toward the nose, is primarily controlled by the medial rectus muscle, one of the six extraocular muscles responsible for eye movement. This muscle originates from the common tendinous ring at the orbital apex and inserts onto the anteromedial surface of the eye, near the cornea. When the medial rectus contracts, it pulls the eye medially, enabling adduction. This action is crucial for binocular vision, allowing both eyes to focus on a single point in the visual field. Coordination with other extraocular muscles ensures smooth and precise eye movements, essential for tasks like reading or tracking objects.
| Characteristics | Values |
|---|---|
| Muscle Name | Medial Rectus Muscle |
| Action | Primary adductor of the eye (moves the eye inward) |
| Innervation | Oculomotor nerve (Cranial Nerve III) |
| Origin | Common tendinous ring (annulus of Zinn) |
| Insertion | Medial aspect of the sclera, about 5.5 mm from the corneal limbus |
| Blood Supply | Ophthalmic artery branches |
| Function | Enables convergence of the eyes for near vision |
| Associated Movement | Adduction (inward movement of the eye) |
| Clinical Significance | Involved in strabismus (e.g., esotropia if overactive, exotropia if underactive) |
| Testing | Assessed during extraocular movement testing (e.g., cover-uncover test) |
Explore related products






What You'll Learn
![]()
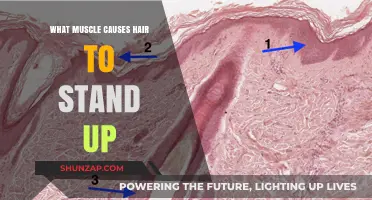
Medial Rectus Muscle Function
The medial rectus muscle is a key player in eye movement, specifically responsible for adduction, the action of moving the eye inward toward the nose. This muscle is one of the six extraocular muscles that control the precise and coordinated movements of the eyeball. When discussing what muscle causes eye adduction, the medial rectus is the primary and most critical muscle involved. Its function is essential for activities such as reading, where both eyes must converge on a near object, and for maintaining binocular vision, which allows for depth perception.
Anatomically, the medial rectus muscle originates from the common tendinous ring (annulus of Zinn) at the orbital apex and inserts into the anteromedial surface of the eyeball. It is innervated by the oculomotor nerve (cranial nerve III), which carries signals from the brainstem to control its contraction. When the medial rectus contracts, it pulls the eye inward along the sagittal plane. This movement is crucial for both voluntary and reflexive eye actions, ensuring that both eyes remain aligned on a single point of focus.
The function of the medial rectus muscle is particularly important in binocular coordination. When both medial rectus muscles contract simultaneously, the eyes converge, allowing for near vision tasks. This convergence is vital for activities like reading or threading a needle, where precise inward movement of both eyes is required. Without proper medial rectus function, individuals may experience diplopia (double vision) or difficulty focusing on close objects, a condition known as convergence insufficiency.
In addition to its role in adduction, the medial rectus muscle works in coordination with other extraocular muscles to ensure smooth and accurate eye movements. For example, during lateral gaze, the medial rectus of one eye must relax while the lateral rectus of the other eye contracts to allow the eyes to move in unison. This coordinated effort is essential for maintaining visual stability and preventing disconjugate gaze, where the eyes do not move together properly.
Clinically, dysfunction of the medial rectus muscle can lead to significant visual impairments. Conditions such as strabismus (misalignment of the eyes) or palsy of the oculomotor nerve can result in impaired adduction, causing the eye to deviate outward. Treatment for such conditions often involves strengthening the medial rectus through exercises or, in severe cases, surgical intervention to realign the muscle. Understanding the medial rectus muscle function is therefore critical for diagnosing and managing disorders related to eye movement and alignment.
In summary, the medial rectus muscle is the primary muscle responsible for eye adduction, playing a central role in both near vision tasks and binocular coordination. Its precise function ensures that the eyes converge accurately, enabling clear and single vision. Whether in everyday activities or specialized tasks, the medial rectus muscle’s role in adduction is indispensable for maintaining optimal visual function.
Nicotine and Muscles: Lactic Acid Buildup Explained
You may want to see also
Explore related products






![]()
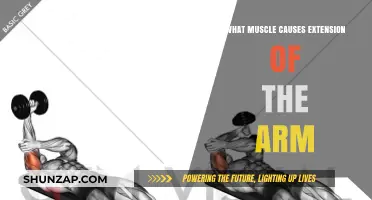
Cranial Nerve VI Role
Cranial Nerve VI, also known as the abducens nerve, plays a crucial role in the lateral movement of the eye, specifically in the action of abduction, which is the outward movement of the eye away from the midline of the face. However, to understand its indirect role in eye adduction (the inward movement of the eye toward the midline), it’s essential to recognize the interplay between the extraocular muscles and cranial nerves. Eye adduction is primarily controlled by the medial rectus muscle, which is innervated by Cranial Nerve III (oculomotor nerve), not Cranial Nerve VI. Despite this, Cranial Nerve VI’s function is vital for coordinated eye movements and maintaining binocular vision.
The primary function of Cranial Nerve VI is to innervate the lateral rectus muscle, which is responsible for abducting the eye. When the lateral rectus muscle contracts, it pulls the eye outward, away from the nose. This action is essential for tasks requiring lateral gaze, such as looking to the side. However, for smooth and coordinated eye movements, the lateral rectus muscle must work in tandem with the medial rectus muscle of the opposite eye. This coordination ensures that both eyes move in unison, allowing for a single, focused image on the retina, a process known as conjugate gaze.
While Cranial Nerve VI does not directly cause eye adduction, its role in abduction is critical for the overall function of eye movement. If Cranial Nerve VI is damaged, such as in cases of abducens nerve palsy, the lateral rectus muscle becomes weak or paralyzed, leading to an inability to abduct the eye. This can result in double vision (diplopia) because the eyes are no longer aligned properly. In such cases, the unaffected medial rectus muscle (innervated by Cranial Nerve III) may still adduct the eye, but the lack of coordinated abduction disrupts normal binocular vision.
Understanding the relationship between Cranial Nerve VI and eye adduction also highlights the importance of neural integration in eye movements. The brainstem nuclei controlling Cranial Nerves III, IV (trochlear nerve), and VI work together to ensure precise and synchronized eye movements. For example, during a leftward gaze, the left lateral rectus muscle (innervated by the left Cranial Nerve VI) abducts the left eye, while the right medial rectus muscle (innervated by the right Cranial Nerve III) adducts the right eye. This coordination is essential for activities like reading or tracking moving objects.
In summary, while Cranial Nerve VI does not directly cause eye adduction, its role in innervating the lateral rectus muscle for abduction is fundamental to the overall mechanics of eye movement. The interplay between Cranial Nerves III and VI ensures that adduction and abduction occur smoothly and in coordination, maintaining proper alignment of the eyes. Damage to Cranial Nerve VI can disrupt this balance, leading to functional impairments and highlighting its indirect but critical role in the complex process of eye movement.
Heart Disease: Muscle Pain as a Warning Sign
You may want to see also
Explore related products






![]()
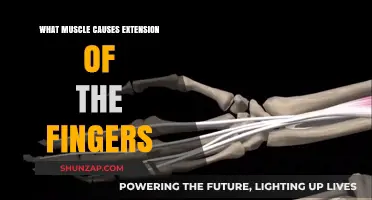
Adduction Movement Mechanics
Eye adduction, the movement of the eye inward toward the nose, is a fundamental action in visual coordination and gaze stabilization. This precise movement is primarily governed by the medial rectus muscle, one of the six extraocular muscles responsible for eye movement. The medial rectus originates from the common tendinous ring (annulus of Zinn) at the orbital apex and inserts onto the anteromedial surface of the eye. When activated, it pulls the eye medially along the transverse axis, enabling adduction. This muscle acts unilaterally; contraction of the medial rectus in one eye produces adduction in that eye alone.
The mechanics of adduction involve a coordinated interplay between neural signals and muscular contraction. Motor control is facilitated by the oculomotor nerve (cranial nerve III), which innervates the medial rectus muscle. When the brain sends a signal to adduct the eye, the oculomotor nerve transmits the impulse to the medial rectus, initiating its contraction. This process is finely tuned to ensure smooth and accurate movement, often in conjunction with other extraocular muscles to maintain binocular alignment and prevent diplopia (double vision).
Biomechanically, the medial rectus operates within the confines of the orbital cavity, where it is supported by fibrous tissue and fat. During adduction, the muscle shortens along its line of pull, exerting a force that rotates the eyeball medially. The range of motion is limited by the muscle's insertion point and the mechanical constraints of the orbit. Overactivity or underactivity of the medial rectus can lead to strabismus, a condition characterized by misaligned eyes, highlighting the importance of balanced muscle function in adduction mechanics.
Adduction is not an isolated movement; it often occurs in conjunction with other ocular motions, such as elevation, depression, or torsion, to achieve a desired gaze direction. For example, during reading, the eyes adduct while also slightly depressing to track text. This coordination is managed by the neural integrator in the brainstem, which maintains the eye's position after a saccadic movement. The integrator ensures that the medial rectus and other extraocular muscles work harmoniously to stabilize the gaze during adduction.
Understanding the mechanics of adduction is crucial in clinical settings, particularly in diagnosing and treating disorders of eye movement. Conditions like medial rectus palsy or internuclear ophthalmoplegia can impair adduction, leading to symptoms such as esotropia (inward deviation of the eye) or impaired convergence. Treatment may involve prism glasses, botulinum toxin injections, or surgical intervention to rebalance muscle forces. By studying the role of the medial rectus in adduction, clinicians can develop targeted therapies to restore normal ocular function.
In summary, adduction movement mechanics are centered on the medial rectus muscle, which acts under the control of the oculomotor nerve to produce inward eye rotation. This process is integrated with other ocular movements and relies on precise neural and biomechanical coordination. Understanding these mechanics not only elucidates normal eye function but also informs the diagnosis and management of adduction-related disorders.
Understanding Back Muscle Atrophy: Causes and Prevention Strategies
You may want to see also
Explore related products






![]()
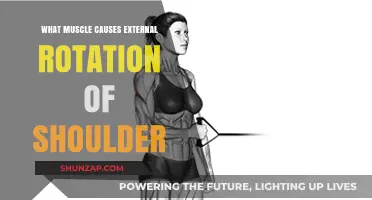
Muscle Innervation Details
The muscle primarily responsible for eye adduction (the movement of the eye inward toward the nose) is the medial rectus muscle. This muscle is one of the six extraocular muscles that control the movements of the eye. Understanding the innervation details of the medial rectus muscle is crucial for comprehending its function and clinical implications.
The medial rectus muscle is innervated by the oculomotor nerve (cranial nerve III). This nerve arises from the oculomotor nucleus located in the midbrain. The oculomotor nerve carries both motor and parasympathetic fibers, but the medial rectus muscle is specifically controlled by the motor fibers. These motor fibers originate in the oculomotor nucleus and travel through the subarachnoid space, the cavernous sinus, and the superior orbital fissure before reaching the medial rectus muscle. The precise innervation ensures coordinated and accurate inward movement of the eye.
The oculomotor nucleus itself receives input from several brain regions, including the supranuclear centers such as the frontal eye fields and the parietal eye fields. These areas are involved in the planning and execution of voluntary eye movements. Additionally, the medial longitudinal fasciculus (MLF) plays a critical role in coordinating conjugate gaze movements, ensuring that both eyes move in unison during adduction. Damage to the MLF can result in internuclear ophthalmoplegia, a condition characterized by impaired adduction of the affected eye.
At the neuromuscular junction, the oculomotor nerve releases the neurotransmitter acetylcholine (ACh) to stimulate muscle contraction in the medial rectus. ACh binds to nicotinic acetylcholine receptors on the muscle fiber, initiating an action potential that leads to muscle fiber contraction. This process is essential for the smooth and precise control of eye adduction. Any disruption in ACh release or receptor function can impair muscle function, leading to conditions such as strabismus or diplopia.
Clinically, understanding the innervation of the medial rectus muscle is vital for diagnosing and managing disorders affecting eye movement. For example, a lesion in the oculomotor nerve can result in a third nerve palsy, characterized by impaired adduction, ptosis, and pupillary dilation. Similarly, conditions such as myasthenia gravis, which affects neuromuscular transmission, can lead to weakness of the medial rectus muscle and subsequent adduction deficits. Thus, knowledge of muscle innervation details is indispensable for both anatomical understanding and clinical practice.
In summary, the medial rectus muscle, responsible for eye adduction, is innervated by the oculomotor nerve (cranial nerve III). This innervation involves a complex pathway from the oculomotor nucleus in the midbrain to the neuromuscular junction, where acetylcholine facilitates muscle contraction. Coordination with supranuclear centers and the medial longitudinal fasciculus ensures precise and conjugate eye movements. Clinical awareness of this innervation is essential for diagnosing and treating disorders related to eye adduction.
Allergies and Muscle Soreness: Is There a Link?
You may want to see also
Explore related products





![RENPHO Eyeris Shift Eye Massager for Migraines [2025 Upgraded], Heated Eye Massager & Sleep Mask for Relaxation, Birthday Gifts for Women/Men/Mom/Dad, Music Temple Fack Mask Massager, Improve Sleep](https://m.media-amazon.com/images/I/610wR-DflgL._AC_UL320_.jpg)
![]()
Clinical Adduction Disorders
The medial rectus muscle is primarily responsible for eye adduction, the movement that turns the eye inward toward the nose. This muscle is one of the six extraocular muscles controlling eye movement and is innervated by the oculomotor nerve (cranial nerve III). When the medial rectus functions properly, it ensures smooth and coordinated inward gaze. However, dysfunction in this muscle or its associated structures can lead to clinical adduction disorders, which manifest as abnormalities in eye alignment and movement.
Another adduction disorder is internuclear ophthalmoplegia (INO), a neurological condition affecting the medial longitudinal fasciculus, a pathway connecting the gaze centers in the brain. INO typically presents as impaired adduction in one eye and nystagmus (involuntary eye movements) in the other eye during lateral gaze. This disorder is often associated with multiple sclerosis, stroke, or other demyelinating diseases. Management focuses on addressing the underlying cause and using prism lenses to manage diplopia.
Duane syndrome is a congenital disorder characterized by abnormal development of the eye muscles, often involving the medial rectus. Patients with Duane syndrome experience limited adduction, accompanied by retraction of the globe and narrowing of the palpebral fissure during attempted adduction. This condition is thought to result from aberrant innervation of the extraocular muscles. Treatment is primarily supportive, with prism glasses or surgery reserved for severe cases.
In addition to these conditions, restrictive adduction disorders can occur due to mechanical limitations, such as scarring or inflammation of the tissues surrounding the medial rectus. Thyroid eye disease, for example, can cause fibrosis and swelling, restricting eye movement. Management may include corticosteroids, orbital decompression surgery, or other interventions to alleviate the mechanical restriction. Understanding the underlying cause of adduction disorders is critical for accurate diagnosis and effective treatment, ensuring optimal visual function and quality of life for patients.
Molecular Mechanisms Behind Acute Muscle Fatigue: Causes and Insights
You may want to see also
Frequently asked questions
The medial rectus muscle is the primary muscle responsible for eye adduction.
The medial rectus muscle contracts to pull the eye inward toward the nose, enabling adduction.
While the medial rectus is the main muscle, the inferior rectus and superior rectus muscles can assist in adduction when the eye is in certain rotated positions.
Weakness or paralysis of the medial rectus muscle results in an inability to adduct the eye, leading to strabismus or a "wall-eyed" appearance.
No, eye adduction cannot occur without the medial rectus muscle, as it is the only muscle with the primary action of pulling the eye inward.