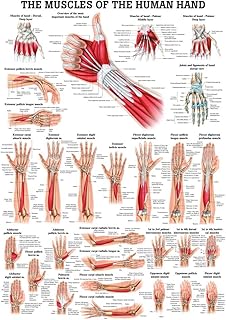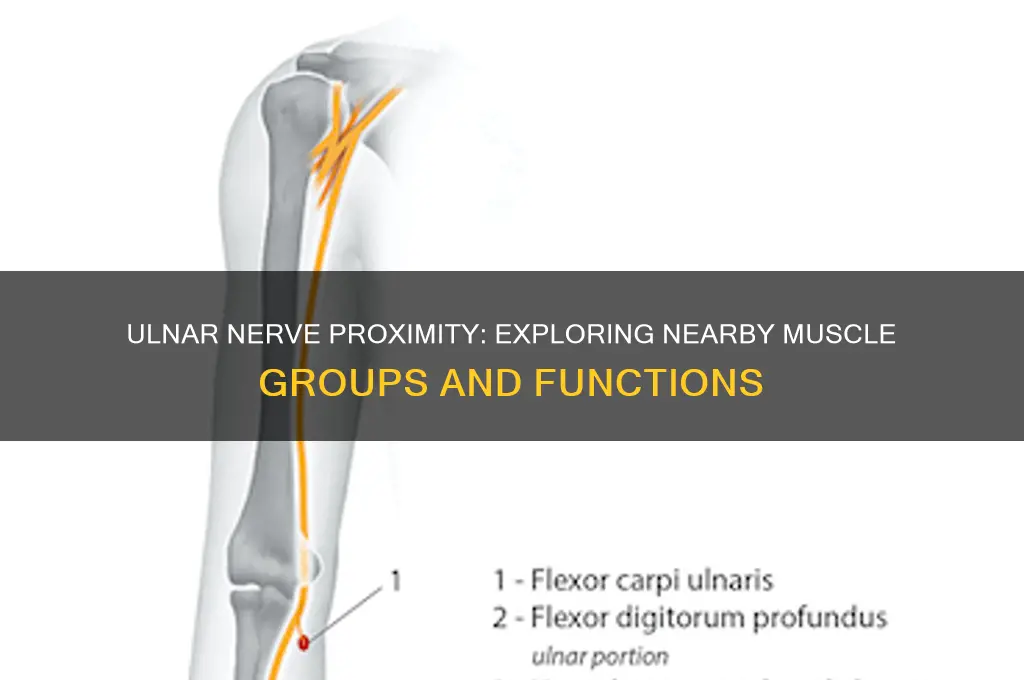
The ulnar nerve, a critical component of the human nervous system, runs along the inner side of the arm and forearm, passing through the elbow and into the hand. It is closely associated with several muscle groups, most notably those in the forearm and hand. Near the ulnar nerve, one can find the flexor carpi ulnaris, which helps in flexing and adducting the wrist, and the flexor digitorum profundus, responsible for flexing the fingers. Additionally, the ulnar nerve innervates the intrinsic muscles of the hand, including the interossei, lumbricals, and hypothenar eminence muscles, which are essential for fine motor control and grip strength. Understanding the proximity of these muscle groups to the ulnar nerve is crucial, as compression or injury to the nerve can lead to symptoms such as numbness, tingling, or weakness in the affected muscles.
| Characteristics | Values |
|---|---|
| Muscle Group | Flexor carpi ulnaris, Flexor digitorum profundus (ulnar half), Palmaris brevis, Hypothenar muscles (Abductor digiti minimi, Flexor digiti minimi brevis, Opponens digiti minimi), Dorsal interossei, 3rd and 4th Lumbricals |
| Nerve Supply | Ulnar nerve (C8-T1) |
| Function | Wrist flexion (ulnar deviation), Finger flexion (ulnar side), Hand abduction/adduction, Grip strength, Fine motor control of fingers |
| Location | Forearm (flexor carpi ulnaris, flexor digitorum profundus), Hand (palmaris brevis, hypothenar muscles, interossei, lumbricals) |
| Clinical Significance | Ulnar nerve compression (e.g., cubital tunnel syndrome) can lead to weakness/wasting of these muscles, causing clawing of the 4th and 5th fingers |
| Blood Supply | Ulnar artery and its branches (e.g., palmar carpal branch, deep palmar arch) |
| Innervation Pattern | Muscles are innervated by the ulnar nerve as it courses through the forearm and hand, with specific branches supplying individual muscles |
| Embryological Origin | Derived from the mesoderm, specifically the somatic mesoderm that forms the limb buds |
| Associated Movements | Ulnar deviation of the wrist, flexion of the ulnar side of the fingers, abduction/adduction of the hand, precision grip |
| Relevant Pathologies | Ulnar nerve palsy, claw hand deformity, hypothenar hammer syndrome, Guyon's canal syndrome |
Explore related products






What You'll Learn
- Forearm Muscles: Flexor carpi ulnaris, flexor digitorum profundus, intrinsic hand muscles
- Ulnar Nerve Path: Runs near medial elbow, forearm, and wrist
- Nerve Entrapment: Cubital tunnel syndrome affects nearby muscles and nerve function
- Hand Grip Strength: Ulnar nerve innervates muscles crucial for fine hand movements
- Adjacent Structures: Pronator quadratus, medial epicondyle, and Guyon's canal proximity
![]()
Forearm Muscles: Flexor carpi ulnaris, flexor digitorum profundus, intrinsic hand muscles
The ulnar nerve, often referred to as the "funny bone," runs along the inner side of the elbow and forearm, supplying sensation and motor function to the hand and forearm muscles. Among the muscles closely associated with this nerve are the flexor carpi ulnaris, flexor digitorum profundus, and the intrinsic hand muscles. These muscles play a critical role in fine motor control, grip strength, and wrist stability, making them essential for daily activities like writing, typing, and lifting objects.
Flexor carpi ulnaris (FCU) is a key muscle in wrist flexion and ulnar deviation, allowing you to bend your wrist and move it toward the little finger side. Located on the ulnar side of the forearm, it is directly innervated by the ulnar nerve. Strengthening the FCU can improve wrist stability and reduce the risk of strain during repetitive tasks. To target this muscle, perform wrist flexion exercises with a dumbbell or resistance band, ensuring you isolate the movement to the ulnar side. Avoid overloading, especially if you have a history of ulnar nerve issues, as excessive strain can exacerbate symptoms like numbness or tingling.
The flexor digitorum profundus (FDP) is another ulnar nerve-innervated muscle, responsible for flexing the distal interphalangeal joints of the fingers. This muscle is crucial for gripping and manipulating objects. Unlike the FCU, the FDP works in tandem with other flexor muscles to produce precise finger movements. To strengthen the FDP, incorporate finger flexion exercises using a hand grip strengthener or resistance bands. For older adults or those recovering from injury, start with low resistance and gradually increase intensity to avoid overloading the ulnar nerve.
The intrinsic hand muscles, including the hypothenar eminence and interossei, are also primarily innervated by the ulnar nerve. These muscles control fine movements of the hand, such as spreading and adducting the fingers. Weakness in these muscles can significantly impair dexterity, making tasks like buttoning shirts or tying shoelaces challenging. To maintain their strength, practice finger abduction and adduction exercises using therapy putty or small objects like marbles. For individuals with ulnar nerve compression (e.g., cubital tunnel syndrome), gentle stretching and nerve gliding exercises can alleviate symptoms while preserving muscle function.
In summary, the ulnar nerve’s proximity to the flexor carpi ulnaris, flexor digitorum profundus, and intrinsic hand muscles underscores their interdependence. Targeted exercises for these muscles not only enhance functional strength but also mitigate the risk of ulnar nerve-related injuries. Whether you’re an athlete, office worker, or senior, incorporating specific movements for these muscles into your routine can improve hand and wrist health, ensuring longevity and precision in your daily activities.
Optimal Rest Days: Timing Your Workouts for Maximum Muscle Growth
You may want to see also
Explore related products





![]()
Ulnar Nerve Path: Runs near medial elbow, forearm, and wrist
The ulnar nerve, often referred to as the "funny bone," follows a distinct path that brings it into close proximity with specific muscle groups in the upper limb. Originating from the brachial plexus, it travels down the arm, hugging the medial (inner) side of the elbow, where it passes through the cubital tunnel. This area is particularly vulnerable to compression, which can cause tingling or numbness in the little and ring fingers. From the elbow, the nerve continues into the forearm, running near the flexor carpi ulnaris muscle, responsible for wrist flexion and ulnar deviation. Finally, it reaches the wrist, passing through the Guyon’s canal alongside the flexor digitorum profundus and the hypothenar muscles, which control fine movements of the hand and grip strength.
Understanding this pathway is crucial for identifying potential injury sites. For instance, prolonged pressure on the elbow, such as leaning on a hard surface, can irritate the ulnar nerve at the cubital tunnel. Similarly, repetitive wrist movements or trauma near Guyon’s canal can lead to ulnar neuropathy, affecting hand dexterity. Athletes, manual laborers, and musicians are particularly at risk due to the repetitive nature of their activities. Practical tips include using elbow pads during prolonged desk work and taking frequent breaks to stretch the forearm and wrist muscles, reducing nerve compression risk.
From an anatomical perspective, the ulnar nerve’s relationship with the flexor carpi ulnaris and hypothenar muscles highlights its role in both gross and fine motor functions. These muscles are innervated by the ulnar nerve, meaning damage to the nerve can result in weakness or paralysis of these groups. For example, a weakened flexor carpi ulnaris may impair the ability to hold a steering wheel or carry groceries. Strengthening these muscles through targeted exercises, such as wrist curls with an ulnar deviation, can improve resilience and reduce injury risk. However, caution should be exercised to avoid overloading the nerve during workouts.
Comparatively, the ulnar nerve’s path contrasts with that of the median nerve, which runs closer to the anterior forearm and innervates different muscle groups. While the median nerve is more commonly associated with carpal tunnel syndrome, ulnar nerve issues often manifest as "claw hand" due to unopposed action of median-innervated muscles. This distinction underscores the importance of precise diagnosis and treatment. For instance, a patient with ulnar nerve compression may benefit from ulnar nerve gliding exercises, whereas median nerve issues might require wrist splinting.
In conclusion, the ulnar nerve’s journey near the medial elbow, forearm, and wrist places it in close contact with critical muscle groups, making it susceptible to compression and injury. Awareness of its path and associated muscles can guide preventive measures and targeted interventions. Whether through ergonomic adjustments, specific exercises, or mindful movement, protecting the ulnar nerve is essential for maintaining hand function and overall upper limb health.
Optimal Muscle Group Spacing: Timing Your Workouts for Maximum Growth
You may want to see also
Explore related products






![]()
Nerve Entrapment: Cubital tunnel syndrome affects nearby muscles and nerve function
The ulnar nerve, often referred to as the "funny bone," runs along the inner side of the elbow and supplies sensation and motor function to the forearm and hand. Nearby muscle groups include the flexor carpi ulnaris, which aids in wrist flexion, and the intrinsic hand muscles responsible for fine finger movements. When this nerve becomes compressed at the elbow—a condition known as cubital tunnel syndrome—it disrupts these muscles' ability to function properly, leading to weakness, numbness, and reduced dexterity.
Consider the mechanics of nerve entrapment: the ulnar nerve passes through a narrow space called the cubital tunnel, where it is vulnerable to pressure from repetitive bending, leaning on the elbow, or anatomical abnormalities. Over time, this compression irritates the nerve, impairing its ability to transmit signals effectively. For instance, prolonged elbow flexion during sleep or activities like cycling can exacerbate the issue. Practical prevention tips include using an elbow pad or adjusting posture to avoid prolonged pressure on the area.
Symptoms of cubital tunnel syndrome often manifest gradually, starting with occasional tingling or numbness in the ring and little fingers. As the condition progresses, individuals may notice muscle atrophy in the hand, particularly in the area between the thumb and index finger, known as the first dorsal interosseous muscle. This weakness can make tasks like gripping objects or typing increasingly difficult. Early intervention, such as physical therapy or bracing, can alleviate symptoms and prevent permanent nerve damage.
Comparing cubital tunnel syndrome to carpal tunnel syndrome highlights the importance of accurate diagnosis. While both conditions involve nerve compression, cubital tunnel affects the ulnar nerve at the elbow, whereas carpal tunnel impacts the median nerve at the wrist. Misdiagnosis can lead to ineffective treatment, such as wrist splinting for a condition rooted in the elbow. A neurologist may perform a nerve conduction study to confirm the location of the entrapment and guide appropriate treatment, which could range from conservative measures to surgical decompression in severe cases.
For those at higher risk—such as individuals with diabetes, thyroid disorders, or occupations requiring repetitive elbow movements—proactive measures are essential. Stretching exercises to maintain elbow flexibility, ergonomic adjustments to reduce pressure on the nerve, and avoiding prolonged elbow flexion can significantly lower the risk of developing cubital tunnel syndrome. Recognizing early signs and seeking timely medical advice can preserve muscle function and prevent long-term complications, ensuring continued hand and arm mobility.
Understanding Collective Action of the Quadriceps Muscle Group
You may want to see also
Explore related products






![]()
Hand Grip Strength: Ulnar nerve innervates muscles crucial for fine hand movements
The ulnar nerve, often referred to as the "funny bone," plays a pivotal role in hand functionality, particularly in fine motor skills and grip strength. This nerve innervates several muscles in the forearm and hand, including the hypothenar eminence and the interossei, which are essential for precise movements like writing, typing, and grasping small objects. Damage or compression of the ulnar nerve, such as in cubital tunnel syndrome, can significantly impair these functions, highlighting its importance in daily activities.
To understand the ulnar nerve's impact on hand grip strength, consider the muscles it directly controls. The flexor carpi ulnaris, for instance, aids in wrist flexion and ulnar deviation, while the dorsal and palmar interossei muscles enable finger abduction and adduction. These movements are critical for maintaining a firm grip and manipulating objects with dexterity. For athletes, musicians, or anyone reliant on hand precision, ulnar nerve health is non-negotiable. Incorporating exercises like finger spreads and grip strengtheners can enhance these muscles, but caution must be taken to avoid overloading the nerve, especially in individuals with pre-existing conditions.
A comparative analysis reveals that ulnar nerve-innervated muscles differ from those controlled by the median or radial nerves in their function and vulnerability. While the median nerve governs primary grip strength via the thenar muscles, the ulnar nerve specializes in finer, more intricate movements. This distinction underscores the need for targeted exercises to maintain balanced hand functionality. For example, squeezing a stress ball primarily engages median nerve muscles, whereas using finger resistance bands activates ulnar nerve-innervated interossei. Combining both approaches ensures comprehensive hand strength development.
Practically, individuals over 40 or those with repetitive strain injuries should prioritize ulnar nerve health. Simple daily habits, such as avoiding prolonged elbow flexion during sleep and taking frequent breaks from gripping tasks, can prevent compression. For those experiencing weakness or numbness, nerve gliding exercises—gently moving the wrist and elbow to mobilize the nerve—can alleviate symptoms. In severe cases, consulting a neurologist or physical therapist is essential, as untreated ulnar nerve issues may lead to irreversible muscle atrophy.
In conclusion, the ulnar nerve’s role in fine hand movements and grip strength is indispensable. By understanding its innervated muscles and implementing targeted exercises and preventive measures, individuals can safeguard their hand functionality. Whether for professional demands or everyday tasks, nurturing ulnar nerve health ensures sustained dexterity and strength, proving that small nerves indeed have a big impact.
Understanding Your Upper Arm: The Major Muscle Group Explained
You may want to see also
Explore related products






![]()
Adjacent Structures: Pronator quadratus, medial epicondyle, and Guyon's canal proximity
The ulnar nerve's journey through the forearm and hand is a complex one, and its proximity to several key structures makes it vulnerable to compression and injury. Among these, the pronator quadratus muscle, the medial epicondyle, and Guyon's canal play significant roles in both function and potential pathology.
Anatomical Proximity and Function
The pronator quadratus, a square-shaped muscle deep in the forearm, lies directly adjacent to the ulnar nerve as it passes through the wrist. This muscle is responsible for pronation (palm-down rotation) of the forearm, a movement essential for activities like typing or turning a doorknob. Its close relationship with the ulnar nerve means that inflammation or hypertrophy of this muscle can compress the nerve, leading to symptoms like numbness or weakness in the hand. For instance, repetitive gripping or twisting motions in occupations such as construction or sports like golf can exacerbate this risk.
The Medial Epicondyle’s Role
At the elbow, the ulnar nerve courses near the medial epicondyle, a bony prominence on the inner side of the humerus. This area, often referred to as the "funny bone," is a common site of ulnar nerve compression, known as cubital tunnel syndrome. The medial epicondyle’s prominence makes the nerve susceptible to pressure, especially during prolonged bending of the elbow or leaning on hard surfaces. Patients with this condition may experience tingling in the ring and little fingers, which can progress to muscle wasting in severe cases. A practical tip: avoid resting your elbow on hard surfaces for extended periods, and consider using a brace to keep the elbow straight during sleep.
Guyon’s Canal: A Critical Passage
As the ulnar nerve enters the hand, it passes through Guyon’s canal, a narrow space bordered by the pisiform bone and the hook of the hamate. This canal is another high-risk area for compression, particularly in cyclists or weightlifters due to prolonged pressure on the heel of the hand. Ulnar nerve entrapment at this site, called Guyon’s canal syndrome, can result in weakness of intrinsic hand muscles and a claw-like deformity of the ring and little fingers. Early intervention, such as modifying grip techniques or using padded gloves, can prevent long-term damage.
Clinical Implications and Prevention
Understanding the proximity of these structures to the ulnar nerve is crucial for both diagnosis and prevention. For example, a patient presenting with hand weakness and numbness should be assessed for activities that involve repetitive elbow bending or wrist pressure. Physical therapy focusing on stretching the pronator quadratus or strengthening the surrounding musculature can alleviate symptoms. In severe cases, surgical decompression at the cubital tunnel or Guyon’s canal may be necessary. A comparative analysis shows that while cubital tunnel syndrome is more common, Guyon’s canal syndrome often presents with more localized and specific symptoms, aiding in differential diagnosis.
Practical Takeaways
To protect the ulnar nerve, consider ergonomic adjustments in daily activities. For desk workers, ensure the elbow is not compressed against hard surfaces. Athletes should use proper padding and vary grip techniques to reduce pressure on Guyon’s canal. Stretching exercises, such as gently rotating the forearm or flexing the wrist, can help maintain nerve mobility. By recognizing the unique vulnerabilities of the ulnar nerve in relation to these adjacent structures, individuals can take proactive steps to prevent injury and maintain hand function.
Understanding Agonist Muscles: Key Roles in Movement and Strength Training
You may want to see also
Frequently asked questions
The ulnar nerve runs close to the flexor carpi ulnaris muscle in the forearm, which is responsible for wrist flexion and ulnar deviation.
Yes, the ulnar nerve innervates the hypothenar muscles in the hand, which control movements of the little finger and the ulnar side of the palm.
The ulnar nerve innervates the medial (ulnar) head of the flexor carpi ulnaris and the flexor digitorum profundus muscles in the forearm.
No, the ulnar nerve does not pass near any muscles in the upper arm; it primarily innervates muscles in the forearm and hand.