
Cranial nerves, a set of 12 paired nerves emerging directly from the brain, play a crucial role in innervating various muscle groups throughout the head, neck, and trunk. These nerves are categorized into sensory, motor, and mixed types, with specific nerves dedicated to controlling distinct muscle functions. For instance, the oculomotor nerve (CN III), trochlear nerve (CN IV), and abducens nerve (CN VI) innervate the extraocular muscles responsible for eye movement, while the trigeminal nerve (CN V) supplies motor function to the muscles of mastication. Additionally, the facial nerve (CN VII) and hypoglossal nerve (CN XII) are vital for facial expressions and tongue movements, respectively. Understanding the specific muscle groups innervated by each cranial nerve is essential for diagnosing and treating neurological disorders affecting these regions.
| Characteristics | Values |
|---|---|
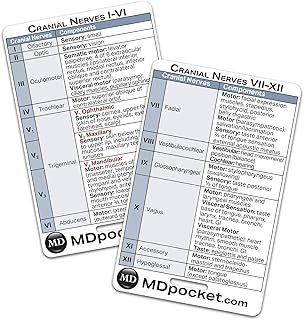
| Cranial Nerve I (Olfactory) | No muscle innervation (sensory nerve for smell) |
| Cranial Nerve II (Optic) | No muscle innervation (sensory nerve for vision) |
| Cranial Nerve III (Oculomotor) | Extraocular muscles (superior, inferior, medial rectus, inferior oblique, and levator palpebrae superioris) |
| Cranial Nerve IV (Trochlear) | Superior oblique muscle of the eye |
| Cranial Nerve V (Trigeminal) | Muscles of mastication (masseter, temporalis, pterygoids, mylohyoid, anterior belly of digastric) |
| Cranial Nerve VI (Abducens) | Lateral rectus muscle of the eye |
| Cranial Nerve VII (Facial) | Muscles of facial expression and stapedius (inner ear) |
| Cranial Nerve VIII (Vestibulocochlear) | No muscle innervation (sensory nerve for hearing and balance) |
| Cranial Nerve IX (Glossopharyngeal) | Stylopharyngeus muscle |
| Cranial Nerve X (Vagus) | Muscles of the pharynx and larynx (except stylopharyngeus) |
| Cranial Nerve XI (Accessory) | Sternocleidomastoid and trapezius muscles |
| Cranial Nerve XII (Hypoglossal) | Muscles of the tongue (intrinsic and extrinsic) |
Explore related products





What You'll Learn
- Oculomotor Nerve (CN III): Innervates extrinsic eye muscles (superior, inferior, medial rectus, inferior oblique, levator palpebrae)
- Trochlear Nerve (CN IV): Supplies superior oblique muscle, controlling downward and outward eye movement
- Abducens Nerve (CN VI): Innervates lateral rectus muscle, enabling outward eye movement (abduction)
- Accessory Nerve (CN XI): Supplies sternocleidomastoid and trapezius muscles, controlling neck and shoulder movements
- Hypoglossal Nerve (CN XII): Innervates intrinsic and extrinsic muscles of the tongue, facilitating tongue movement
![]()
Oculomotor Nerve (CN III): Innervates extrinsic eye muscles (superior, inferior, medial rectus, inferior oblique, levator palpebrae)
The oculomotor nerve, or CN III, is a powerhouse of ocular control, innervating five of the six extrinsic eye muscles responsible for gaze stabilization and visual tracking. These muscles—superior rectus, inferior rectus, medial rectus, inferior oblique, and levator palpebrae superioris—work in concert to enable precise eye movements, from reading fine print to tracking a moving object. Understanding CN III’s role is critical for diagnosing conditions like oculomotor nerve palsy, where paralysis of these muscles results in double vision, drooping eyelids, or inability to move the eye in specific directions.
Analyzing the function of each muscle reveals CN III’s complexity. The superior rectus elevates and intorts the eye, while the inferior rectus depresses and extorts it. The medial rectus adducts the eye, and the inferior oblique primarily extorts and elevates it. The levator palpebrae superioris, though not directly involved in eye movement, lifts the upper eyelid, ensuring the visual field remains unobstructed. Damage to CN III can thus impair both gaze direction and eyelid position, highlighting its dual role in vision and facial aesthetics.
Clinicians often assess CN III function through specific tests. For instance, asking a patient to follow a moving target in all directions evaluates the rectus and oblique muscles, while observing eyelid position at rest and during upward gaze tests the levator palpebrae. In cases of suspected CN III palsy, imaging studies like MRI or CT scans may be ordered to identify compressive lesions, such as aneurysms or tumors, which commonly affect this nerve due to its proximity to the brainstem and subarachnoid space.
Practical tips for patients with CN III dysfunction include prism glasses to alleviate double vision and eyelid crutches for ptosis management. Physical therapy, focusing on compensatory head movements, can also improve quality of life. For example, a patient with a weak medial rectus might turn their head to the side to align their eyes, reducing diplopia. Early intervention is key, as prolonged misalignment can lead to amblyopia or permanent vision loss in severe cases.
In summary, the oculomotor nerve’s innervation of the extrinsic eye muscles and levator palpebrae superioris is essential for both visual function and facial appearance. Its vulnerability to compression and ischemia underscores the importance of prompt evaluation and targeted management. Whether through clinical testing, imaging, or rehabilitative strategies, addressing CN III dysfunction requires a nuanced understanding of its unique anatomical and functional contributions.
Effective Muscle Group Splits for Optimal Lifting Results and Recovery
You may want to see also
Explore related products






![]()
Trochlear Nerve (CN IV): Supplies superior oblique muscle, controlling downward and outward eye movement
The trochlear nerve, or CN IV, is a fascinating component of the cranial nerve system, primarily due to its unique path and function. Unlike other cranial nerves that emerge from the brainstem, the trochlear nerve exits from the dorsal aspect of the brainstem, crosses to the opposite side, and then travels a considerable distance to innervate its target muscle. This nerve is solely responsible for supplying the superior oblique muscle, one of the six extraocular muscles that control eye movement. Understanding its role is crucial for diagnosing and treating conditions related to eye motility.
From an anatomical perspective, the superior oblique muscle plays a pivotal role in eye movement, specifically in depression, abduction, and intorsion of the eyeball. When the trochlear nerve is functioning correctly, it allows for smooth, coordinated downward and outward eye movements, essential for activities like reading or looking at objects below eye level. For instance, when you tilt your head to the right and look down, the superior oblique muscle on the left side contracts, facilitated by the trochlear nerve, to stabilize and align the eyes properly. This coordination is vital for maintaining binocular vision and depth perception.
Clinically, damage to the trochlear nerve can lead to vertical diplopia, or double vision, particularly when looking downward. This condition often results from trauma, such as a head injury, or neurological disorders like multiple sclerosis. Diagnosis typically involves a thorough eye examination, including the assessment of eye movement and pupil response. Treatment may range from prism glasses to correct double vision, to surgical intervention in severe cases. For example, a 45-year-old patient with a history of a car accident might present with vertical diplopia due to a trochlear nerve injury, requiring a combination of physical therapy and corrective lenses to manage symptoms.
To prevent complications related to trochlear nerve dysfunction, it’s essential to protect the head from injury, especially in high-risk activities like sports or construction work. Wearing helmets and seatbelts can significantly reduce the likelihood of trauma affecting the nerve. Additionally, maintaining overall neurological health through a balanced diet, regular exercise, and managing conditions like diabetes or hypertension can help preserve cranial nerve function. For those experiencing symptoms of double vision or eye misalignment, seeking prompt medical attention is critical to prevent long-term visual impairment.
In summary, the trochlear nerve’s role in innervating the superior oblique muscle underscores its importance in precise eye movement and visual coordination. Its unique anatomical pathway and specific function make it a critical yet vulnerable component of the cranial nerve system. By understanding its role and taking preventive measures, individuals can safeguard their visual health and address potential issues before they escalate. Whether through protective gear or timely medical intervention, prioritizing the health of the trochlear nerve is essential for maintaining optimal vision.
Optimal Sets for Small Muscle Groups: Maximizing Growth and Strength
You may want to see also
Explore related products






![]()
Abducens Nerve (CN VI): Innervates lateral rectus muscle, enabling outward eye movement (abduction)
The abducens nerve, or cranial nerve VI, plays a precise and critical role in ocular motility. It exclusively innervates the lateral rectus muscle, one of the six extraocular muscles responsible for eye movement. This specialization allows for a singular function: the abduction of the eye, or its outward movement away from the midline of the face. This action is essential for tasks requiring peripheral vision, such as reading, driving, or scanning a landscape. Without the abducens nerve, the ability to look laterally would be severely compromised, leading to diplopia (double vision) and significant visual impairment.
To understand the abducens nerve’s importance, consider its anatomical pathway. Originating in the pons of the brainstem, it travels through the cavernous sinus before reaching the lateral rectus muscle. This long course makes it vulnerable to damage from trauma, tumors, or increased intracranial pressure, which can result in abducens nerve palsy. Symptoms of palsy include horizontal diplopia, a head tilt toward the affected side (to compensate for the inability to abduct the eye), and difficulty with activities requiring lateral gaze. Early diagnosis and treatment, often involving prism glasses or botulinum toxin injections, are crucial to managing these symptoms effectively.
Clinically, assessing the abducens nerve is straightforward. During a neurological exam, patients are instructed to follow a moving target with their eyes, such as a pen or finger, while the examiner observes for limitations in lateral gaze. Weakness or paralysis of the lateral rectus muscle is a telltale sign of abducens nerve dysfunction. In children, congenital abnormalities of this nerve are rare but can be identified through similar testing, often requiring surgical intervention to correct misalignment and restore binocular vision.
For those with abducens nerve palsy, practical tips can improve daily functioning. Patching one eye can alleviate double vision temporarily, though this should be used sparingly to avoid disuse of the affected eye. Physical therapy exercises, such as pencil push-ups or Brock string exercises, may help strengthen eye muscles and improve coordination. Additionally, avoiding activities that strain the eyes, like prolonged screen time, can reduce discomfort. In severe cases, surgical options like lateral rectus muscle recession or resection may be considered to realign the eyes and restore proper function.
In summary, the abducens nerve’s singular focus on the lateral rectus muscle underscores its unique role in ocular movement. Its vulnerability to damage highlights the need for prompt evaluation and management of related disorders. By understanding its function and clinical implications, healthcare providers and patients alike can take proactive steps to preserve vision and quality of life. Whether through conservative measures or surgical intervention, addressing abducens nerve dysfunction is key to maintaining optimal eye health.
Is Weekly Muscle Group Training Sufficient for Optimal Growth?
You may want to see also
Explore related products






![]()
Accessory Nerve (CN XI): Supplies sternocleidomastoid and trapezius muscles, controlling neck and shoulder movements
The accessory nerve, or cranial nerve XI, plays a pivotal role in our ability to move and stabilize the neck and shoulders. It is one of the few cranial nerves primarily dedicated to motor function, innervating two key muscles: the sternocleidomastoid and the trapezius. These muscles are essential for everyday activities, from turning your head to shrugging your shoulders, making the accessory nerve a critical component of upper body mobility.
Function and Anatomy
The sternocleidomastoid muscle, a strap-like structure running from the sternum and clavicle to the mastoid process of the skull, is responsible for rotating and flexing the neck. When both sides contract, it flexes the neck forward; when one side contracts, it rotates the head to the opposite side. The trapezius, a large, flat muscle extending from the occipital bone to the lower thoracic spine and clavicle, stabilizes and moves the scapula. It enables actions like shrugging, retracting, and depressing the shoulders, as well as extending and laterally flexing the neck. Together, these muscles ensure precise control over neck and shoulder movements, highlighting the accessory nerve’s specialized role.
Clinical Relevance and Testing
Damage to the accessory nerve can result in noticeable deficits. Weakness in the sternocleidomastoid may cause difficulty turning the head, while trapezius impairment can lead to shoulder drooping and scapular winging. Clinicians test CN XI function by asking patients to rotate their head against resistance or shrug their shoulders. For a more precise assessment, electromyography (EMG) or nerve conduction studies can be performed to evaluate nerve integrity. Early detection of accessory nerve dysfunction is crucial, as it may indicate underlying conditions like trauma, tumors, or neurological disorders.
Practical Tips for Strengthening and Protecting CN XI
To maintain the health of the accessory nerve and its target muscles, incorporate targeted exercises into your routine. Neck rotations, shoulder shrugs, and scapular retractions (e.g., pulling your shoulder blades together) can strengthen the sternocleidomastoid and trapezius. When lifting heavy objects, ensure proper posture to avoid straining these muscles. For individuals recovering from nerve injury, physical therapy with a focus on gradual resistance training can aid in restoring function. Always avoid sudden, jerky movements that could stress the neck and shoulders, as these can exacerbate nerve damage.
Comparative Insight
Unlike other cranial nerves that innervate multiple muscle groups or serve dual sensory and motor functions, the accessory nerve is almost exclusively motor-focused. Its unique pathway—exiting the skull through the jugular foramen and traveling alongside the vagus nerve—underscores its specialized role. While it shares some similarities with the hypoglossal nerve (CN XII) in its motor function, the accessory nerve’s influence on the upper body distinguishes it as a key player in postural stability and movement. Understanding this distinction is essential for both anatomical study and clinical practice.
Understanding the Muscle Group Surrounding the Ulna: Anatomy Explained
You may want to see also
Explore related products






![]()
Hypoglossal Nerve (CN XII): Innervates intrinsic and extrinsic muscles of the tongue, facilitating tongue movement
The hypoglossal nerve, or cranial nerve XII, is the unsung hero of articulation, swallowing, and even the subtle act of tasting. It exclusively innervates the muscles responsible for tongue movement, both intrinsic (within the tongue) and extrinsic (outside the tongue). This specialization makes it unique among cranial nerves, as it doesn’t branch into sensory or other motor functions. Damage to the hypoglossal nerve can lead to profound difficulties in speech and eating, underscoring its critical role in daily life.
To understand its function, consider the tongue’s complexity. The intrinsic muscles (longitudinalis, transversus, verticalis) alter the tongue’s shape, allowing it to curl, flatten, or form a groove. The extrinsic muscles (genioglossus, hyoglossus, styloglossus, palatoglossus) move the tongue as a whole—protruding it, retracting it, or shifting it side to side. The hypoglossal nerve orchestrates these movements bilaterally, with the left and right nerves controlling muscles on their respective sides. This precise coordination is why a unilateral injury (e.g., from a stroke) results in tongue deviation toward the affected side when protruded.
Clinicians assess hypoglossal nerve function through simple tests: asking patients to protrude their tongue and observing for deviation, weakness, or atrophy. For example, in a 65-year-old patient with a suspected stroke, a deviated tongue could indicate damage to the nerve’s pathway. Rehabilitation strategies often include tongue-strengthening exercises, such as pressing the tongue against the roof of the mouth for 5–10 seconds, repeated 10–15 times daily. Speech therapists may also incorporate articulation drills to retrain precise movements.
Comparatively, while other cranial nerves (e.g., the facial nerve, CN VII) innervate multiple muscle groups and sensory functions, the hypoglossal nerve’s singular focus on tongue musculature makes it diagnostically straightforward. However, this specificity means its impairment has immediate, noticeable consequences. For instance, a child with a congenital hypoglossal nerve anomaly might struggle with breastfeeding due to poor tongue control, requiring early intervention with feeding specialists.
In summary, the hypoglossal nerve’s role in tongue mobility is both specialized and indispensable. Its function can be assessed through simple clinical tests, and rehabilitation strategies are tailored to restore or compensate for lost movement. Understanding its unique anatomy and impact highlights the intricate relationship between neural innervation and everyday activities like speaking and eating.
Optimal Muscle Group Split: Maximizing Gains and Recovery Efficiently
You may want to see also
Frequently asked questions
The cranial nerves innervate various muscle groups, including those of the face, neck, eyes, tongue, pharynx, larynx, and extraocular muscles.
The facial nerve (cranial nerve VII) innervates the muscles of facial expression, such as those responsible for smiling, frowning, and closing the eyes.
The oculomotor nerve innervates most of the extraocular muscles (superior, inferior, and medial rectus; inferior oblique) and the levator palpebrae superioris, which controls eyelid elevation.
The trigeminal nerve (cranial nerve V) innervates the muscles of mastication, including the temporalis, masseter, medial pterygoid, and lateral pterygoid muscles.































