Lateral Femoral Cutaneous Nerve (LFCN) is a pure sensory nerve that arises from the lumbar plexus. It travels downward lateral to the psoas muscle, passes through or underneath the inguinal ligament, and innervates the lateral thigh. The LFCN has two terminal divisions, anterior and lateral, which carry sensory information from the anterolateral thigh and buttock. LFCN entrapment, also known as Meralgia Paresthetica, can cause pain, burning, tingling, numbness, and coldness on the front side of the thigh.
| Characteristics | Values |
|---|---|
| Full Form | Lateral Femoral Cutaneous Nerve |
| Type | Purely Sensory |
| Origin | L2 and L3 nerves of the lumbar plexus |
| Variation | Arises from L1 and L2 ("high form") and from L3 and L4 ("low form") |
| Exit Point | Underneath the inguinal ligament, medial to ASIS by 1-2 cm |
| Entrapment Syndrome | Meralgia Paresthetica |
| Symptoms | Pain, burning, tingling, numbness, coldness, hypersensitivity, or buzzing on the front side of the thigh |
| Treatment | Cortisone injection, heat treatment, pulsed radiofrequency neurotomy, strapping, massage, manual therapy, acupuncture, weight loss |
Explore related products






What You'll Learn
![]()
LFCN is a sensory nerve
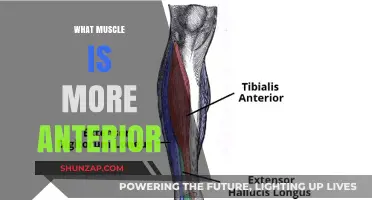
The Lateral Femoral Cutaneous Nerve (LFCN) is a sensory nerve that supplies the parietal peritoneum in the iliac fossa and the skin on the anterolateral and lateral surfaces of the thigh. It is derived from the posterior divisions of the L2 and L3 nerves of the lumbar plexus. The LFCN has two terminal divisions, anterior and lateral, which carry sensory information from respective areas of the anterolateral thigh and buttock.
The LFCN is a small nerve that can be challenging to locate and identify, especially near the anterior superior iliac spine (ASIS). It lies on the surface of the sartorius muscle and, as it traverses caudally, it tends to lie in the groove between the sartorius muscle and tensor fascia lata muscle. The nerve is usually 1-2 mm thick and can be visualised using ultrasound.
The LFCN passes under the inguinal ligament to reach the thigh, where it divides into anterior and posterior branches. The anterior branch becomes superficial about 10 cm below the inguinal ligament and divides into branches that are distributed to the skin of the anterior and lateral parts of the thigh, as far down as the knee. The posterior branch pierces the fascia lata and subdivides into filaments, which pass backward across the lateral and posterior surfaces of the thigh, supplying the skin around the greater trochanter.
Entrapment of the LFCN can cause meralgia paresthetica (Bernhardt-Roth syndrome), a condition characterised by pain, burning, tingling, numbness, coldness, hypersensitivity, or buzzing on the front side of the thigh. This can be caused by tight-fitting clothing, excessive weight gain, and obesity. Diagnosis of meralgia paresthetica is based on a thorough subjective and physical examination, and treatment options include weight loss advice, cortisone injections, and desensitisation of the nerve using heat treatment or pulsed radiofrequency neurotomy.
Flexeril: Muscle Relaxant and Spasm Solution
You may want to see also
Explore related products

![Nerve [Blu-ray + DVD + Digital HD]](https://m.media-amazon.com/images/I/511M7e90gSL._AC_UY218_.jpg)




![]()
It arises from L2 and L3 nerves
The Lateral Femoral Cutaneous Nerve (LFCN) is a purely sensory nerve that supplies the parietal peritoneum in the iliac fossa and the anterior and lateral surfaces of the thigh. It is also known as the lateral cutaneous nerve of the thigh. Typically, the LFCN arises from the posterior or dorsal divisions of the L2 and L3 nerves of the lumbar plexus. However, there are anatomical variations, with the LFCN also potentially arising from L1 and L2 ("high form") or L3 and L4 ("low form").
The LFCN is of interest to many types of surgeons due to its anatomical variations and the potential for iatrogenic injury during surgical procedures. The nerve typically emerges from the lateral border of the psoas major muscle, travelling obliquely within a duplication of the fascia iliaca, towards the anterior superior iliac spine (ASIS). It then exits the pelvis and enters the anterolateral aspect of the thigh, where it divides into anterior and posterior branches. The anterior branch provides sensory innervation to the skin of the anterolateral thigh down to the knee, while the posterior branch pierces through the fascia lata and divides to provide innervation to the lateral skin and, occasionally, the gluteal skin.
The L2 and L3 nerves, from which the LFCN typically arises, are spinal nerves that provide sensation to the front part of the thigh and the inner side of the lower leg. They also control movements of the hip and knee muscles. The LFCN, as a purely sensory nerve, does not cause motor weakness or wasting, but conditions such as meralgia paresthetica can cause pain, burning, tingling, numbness, and other uncomfortable sensations in the thigh.
The LFCN's proximity to the hip and thigh means that it can be affected by prolonged standing and extension at the hip joint, with symptoms relieved to some extent by sitting or hip flexion. Various treatments for LFCN entrapment exist, including cortisone injections, desensitisation of the nerve using heat treatment, and pulsed radiofrequency neurotomy.
Piriformis Muscle Syndrome: Understanding the Pain and Treatment
You may want to see also
Explore related products





![]()
It passes through the psoas major muscle
The Lateral Femoral Cutaneous Nerve (LFCN) is a pure sensory nerve that carries sensory information from the anterolateral thigh and buttock. In its most typical course, it emerges at the lateral aspect of the psoas major muscle, a long, ribbon-shaped core muscle in the back, and travels obliquely within a duplication of the fascia iliaca. The psoas major muscle is one of two psoas muscles that sit on either side of the spine, starting in the lower back just below the ribs and running through the pelvis to the top of the femur (thigh bone).
The psoas major muscle is closely related to a number of retroperitoneal structures, including the kidneys, ureters, gonadal vessels, and the genitofemoral nerve. The lumbar plexus, from which the LFCN is derived, is embedded in the psoas major as it exits the vertebral canal. The psoas major also contributes to the floor of the femoral triangle in the thigh.
The psoas major muscle functions as both a static and dynamic muscle, assisting with lateral motions and stabilising the lumbar spine when in a static position. It acts as a hip flexor, hip adductor, and hip external rotator, and its tendon (iliopsoas tendon) lies deep to the fascia lata, sartorius, rectus femoris, and deep femoral artery.
The LFCN typically exits the pelvis and enters the anterolateral thigh, where it divides into anterior and posterior branches. The anterior branch provides sensory innervation to the skin of the anterolateral thigh down to the knee, while the posterior branch pierces through the fascia lata and divides to provide innervation to the lateral skin and, occasionally, the gluteal skin.
The LFCN is of interest to many types of surgeons due to its anatomical variations, which occur in up to 18% of cases. Knowledge of these variations is essential to avoid iatrogenic complications during surgical procedures.
Barbell Row: Building a Strong Back
You may want to see also
![]()
LFCN exits the pelvis and enters the thigh
The Lateral Femoral Cutaneous Nerve (LFCN) is a pure sensory nerve that carries afferent sensory fibres. It is usually derived from the dorsal branches of the L2 and L3 ventral rami. It can also emerge from the femoral nerve or as a distinct branch of the lumbar plexus.
The LFCN exits the pelvis and enters the thigh region, usually medial to the ASIS (anterior superior iliac spine) and underneath the inguinal ligament. However, there are significant variations to this anatomical course. Cadaveric studies have distinguished five categories of anatomical variation in the LFCN's exit from the pelvis and entry to the thigh. The nerve has been observed exiting the pelvis in seven different locations in relation to the inguinal ligament and ASIS. It typically exits medial to the ASIS and under the inguinal ligament, but it has also been seen exiting superior or lateral to the ASIS.
The LFCN emerges at the lateral aspect of the psoas major muscle, travelling obliquely within a duplication of the fascia iliaca towards the ASIS. It then passes through the inguinal ligament, where it is flattened and encompassed by a concentrically arranged thick perineurium. The mean distance from the ASIS to the point where the LFCN passes through the inguinal ligament is 1.87 ± 0.48 cm.
During its descent through the thigh, the LFCN divides into anterior and posterior branches. The anterior branch becomes superficial at a point 10 cm distal to the ASIS, providing sensory innervation to the skin of the anterolateral thigh down to the knee. The posterior branch pierces through the fascia lata at a higher point than the anterior branch and further divides to innervate the lateral skin from the greater trochanter to the mid-thigh, sometimes extending to the gluteal skin.
The Muscle Man: Farris' Fitness Journey
You may want to see also
![]()
It divides into anterior and posterior branches
The Lateral Femoral Cutaneous Nerve (LFCN) is a purely sensory nerve that arises from the posterior divisions of the L2 and L3 nerves of the lumbar plexus. It can also emerge from the femoral nerve or as a distinct branch of the lumbar plexus.
The LFCN travels downward, lateral to the psoas muscle, and crosses the iliacus muscle (deep to fascia). It then passes through or underneath the lateral aspect of the inguinal ligament and finally travels to innervate the lateral thigh.
During its descent through the thigh, the LFCN divides into anterior and posterior branches. At a point 10 cm distal to the anterior superior iliac spine (ASIS), its anterior branch becomes superficial and provides sensory innervation to the skin of the anterolateral thigh down to the knee. The anterior branch also connects with cutaneous branches of the anterior femoral nerve and the infrapatellar branch of the saphenous nerve to form the peripatellar plexus.
The posterior branch pierces through the fascia lata at a point higher than the anterior branch and further divides to provide innervation to the lateral skin from the greater trochanter to mid-distance along the thigh. It can also supply the gluteal skin.
The LFCN is of interest not only to nerve surgeons but also to laparoscopic surgeons, bariatric surgeons, general surgeons, orthopedists, and spine surgeons due to its anatomical variations and the potential for iatrogenic injury during surgical procedures.
Sim Characters and Their Muscle Memory Loss
You may want to see also
Frequently asked questions
The Lateral Femoral Cutaneous Nerve (LFCN) is a purely sensory nerve that arises from the lumbar plexus.
The LFCN provides sensory innervation to the lateral thigh. It carries sensory information from the anterolateral thigh and buttock.
The LFCN arises from the posterior divisions of L2 and L3, travels downward lateral to the psoas muscle, passes through or underneath the inguinal ligament, and divides into anterior and posterior branches.
LFCN entrapment, also known as Meralgia Paresthetica, is a condition where the LFCN becomes compressed or entrapped, causing symptoms such as pain, burning, tingling, and numbness on the front side of the thigh.