Passive external rotation of the arm primarily involves the subscapularis muscle, which is part of the rotator cuff and plays a crucial role in stabilizing the shoulder joint. During passive external rotation, the subscapularis is in a lengthened, or stretched, position, allowing the humerus to rotate outward relative to the shoulder. This movement is often facilitated by external forces, such as gravity or manual assistance, rather than active muscle contraction. Understanding the role of the subscapularis in this motion is essential for assessing shoulder function, diagnosing injuries, and designing rehabilitation programs for conditions like rotator cuff tears or shoulder impingement.
Explore related products





What You'll Learn
- Infraspinatus Role: Infraspinatus stabilizes shoulder, allows passive external rotation when relaxed
- Posterior Capsule: Tight posterior capsule restricts passive external rotation range
- Subscapularis Inhibition: Weak or inhibited subscapularis can increase passive external rotation
- Joint Laxity: Hypermobile shoulders often exhibit greater passive external rotation
- Rotator Cuff Balance: Imbalanced rotator cuff muscles affect passive external rotation
![]()
Infraspinatus Role: Infraspinatus stabilizes shoulder, allows passive external rotation when relaxed
The infraspinatus muscle, nestled within the scapula's infraspinous fossa, plays a pivotal role in shoulder function. While its primary function is external rotation of the arm, a lesser-known yet crucial aspect is its contribution to passive external rotation when in a relaxed state. This occurs due to the muscle's tonic activity, which provides a baseline tension even at rest, allowing the arm to maintain a slight outward rotation without active engagement.
To understand this mechanism, consider the infraspinatus as a stabilizer rather than just a mover. When the muscle is relaxed, its residual tension acts as a counterbalance to internal rotators like the subscapularis, preventing the arm from collapsing inward. This passive external rotation is particularly evident when the arm is at rest by the side or during activities like reaching behind the back. For instance, athletes in sports requiring overhead motions, such as tennis or swimming, rely on this passive stability to maintain proper shoulder alignment and reduce injury risk.
Clinically, assessing passive external rotation can provide insights into infraspinatus health. A significant loss of this range of motion may indicate tightness, weakness, or injury to the muscle or its tendon. Physical therapists often use this assessment to diagnose conditions like rotator cuff tendinopathy or impingement syndrome. To enhance infraspinatus function, targeted exercises such as external rotation with a resistance band (3 sets of 12–15 reps, 2–3 times weekly) can strengthen the muscle, while cross-body stretches (hold for 30 seconds, repeat 3 times daily) improve flexibility and maintain passive rotation.
Comparatively, while the infraspinatus is not the sole contributor to passive external rotation—the teres minor and joint capsule also play roles—its position and size make it the primary stabilizer in this context. Unlike active external rotation, which requires muscle contraction, passive rotation relies on the infraspinatus’s ability to maintain tone without fatigue, highlighting its unique anatomical design.
In practical terms, individuals experiencing shoulder stiffness or pain should focus on exercises that mimic the infraspinatus’s passive role. For example, sleeping with a pillow between the arm and torso can encourage external rotation during rest, promoting healing and reducing strain. Additionally, incorporating isometric holds (e.g., holding a doorframe with the arm externally rotated for 10 seconds, repeated 5 times) can enhance stability without overloading the muscle. By understanding and addressing the infraspinatus’s passive function, one can optimize shoulder health and prevent long-term dysfunction.
Understanding the Muscles Responsible for Holding Your Arm Soutward
You may want to see also
Explore related products






![]()
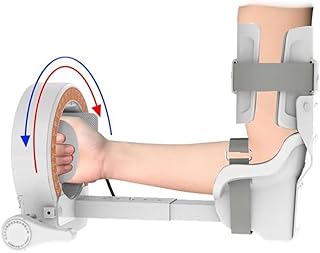
Posterior Capsule: Tight posterior capsule restricts passive external rotation range
The posterior capsule of the shoulder joint is a critical yet often overlooked structure in discussions about arm mobility. When this tissue becomes tight, it can significantly limit passive external rotation—a movement essential for activities like reaching behind the back or throwing a ball. This restriction is not merely a matter of flexibility but a complex interplay of anatomy, biomechanics, and functional demands. Understanding this relationship is key to addressing mobility issues effectively.
Consider the mechanics: during passive external rotation, the arm is moved by an external force while the muscles remain relaxed. The posterior capsule, located at the back of the shoulder joint, acts as a barrier to this motion. When it tightens—often due to overuse, injury, or prolonged immobility—it physically restricts the humeral head’s ability to rotate outward. This tightness is commonly seen in athletes, particularly throwers or swimmers, and in individuals with adhesive capsulitis (frozen shoulder). A simple test to assess this restriction involves lying on your back with your arm at 90 degrees abduction and allowing someone to gently rotate your arm outward, noting any resistance or end-range discomfort.
Addressing a tight posterior capsule requires targeted intervention. Stretching alone may not suffice; the tissue’s adaptability is influenced by its collagen composition and neural tension. A proven approach is the sleeper stretch: lie on the affected side with your arm at 90 degrees, then gently externally rotate your arm toward the bed, holding for 30–60 seconds, repeated 3–4 times daily. For severe cases, manual therapy from a physical therapist can help mobilize the capsule, often using techniques like posterior glide or distraction. Caution: aggressive stretching without proper assessment can exacerbate inflammation or instability, particularly in hypermobile individuals.
Comparatively, active external rotation—where muscles like the infraspinatus and teres minor engage—is less affected by posterior capsule tightness. However, passive range limitations often correlate with functional deficits, such as difficulty in sports or daily tasks. A holistic approach, combining mobility work with strength training for the rotator cuff, ensures stability alongside flexibility. For instance, incorporating band pull-aparts or prone horizontal abduction exercises can balance the forces acting on the shoulder, reducing undue stress on the capsule.
In conclusion, a tight posterior capsule is a specific yet impactful contributor to restricted passive external rotation. Recognizing its role allows for precise interventions, from targeted stretches to professional manual therapy. By addressing this structure, individuals can restore not just range of motion but also the functional capacity needed for both athletic performance and everyday activities. Always assess movement patterns and seek professional guidance when in doubt, as the shoulder’s complexity demands a nuanced approach.
Are Arm Muscles Red? Unveiling the Truth Behind Muscle Color
You may want to see also
Explore related products






![]()
Subscapularis Inhibition: Weak or inhibited subscapularis can increase passive external rotation
The subscapularis muscle, a key player in shoulder stability and movement, often goes unnoticed until its dysfunction becomes apparent. When this muscle is weak or inhibited, it can lead to an unexpected outcome: increased passive external rotation of the arm. This phenomenon is not merely a curiosity but a critical insight for understanding shoulder mechanics and addressing related issues.
Understanding the Mechanism
Passive external rotation occurs when the arm is rotated outward without active muscle engagement, relying instead on the flexibility and balance of surrounding structures. The subscapularis, located at the front of the shoulder blade, internally rotates the arm and stabilizes the humeral head. When it is weak or inhibited, its counterforce to external rotation diminishes, allowing the arm to rotate outward more freely. This imbalance often stems from prolonged postures, overuse, or injury, particularly in athletes or individuals with desk jobs.
Practical Implications and Assessment
To identify subscapularis inhibition, clinicians often perform the "belly press test" or "lift-off test," where difficulty in pressing the hand against the belly or lifting the hand away from the back indicates weakness. For self-assessment, try this: stand with your arm at your side, elbow bent at 90 degrees, and attempt to internally rotate your arm against resistance. Weakness or pain suggests subscapularis dysfunction. Addressing this issue early can prevent compensatory patterns that lead to impingement or rotator cuff injuries.
Corrective Strategies
Strengthening the subscapularis is paramount. Exercises like the "wall slide with internal rotation" or "band pull-apart" can restore balance. For the wall slide, stand facing a wall, place your forearm against it with your elbow at 90 degrees, and slide your arm upward while keeping contact with the wall. Aim for 3 sets of 10–15 repetitions daily. Additionally, manual therapy or foam rolling can alleviate tightness in the posterior shoulder, further enhancing subscapularis function.
Prevention and Long-Term Management
Incorporating shoulder mobility drills into daily routines is essential, especially for those in sedentary or repetitive occupations. Stretching the posterior capsule with a "sleeper stretch" (lying on the affected side, bending the elbow at 90 degrees, and gently pushing the forearm toward the floor) can complement subscapularis strengthening. Consistency is key; neglecting these practices can perpetuate the imbalance, leading to chronic issues. For athletes, integrating these exercises into warm-up routines can reduce injury risk and optimize performance.
By recognizing the role of subscapularis inhibition in passive external rotation, individuals can take proactive steps to restore shoulder health, ensuring both stability and mobility in their daily lives.
Correct Left Arm Muscle Imbalance: Effective Exercises and Techniques
You may want to see also
Explore related products




![]()
Joint Laxity: Hypermobile shoulders often exhibit greater passive external rotation
Hypermobile shoulders, characterized by joint laxity, often demonstrate a notable increase in passive external rotation. This phenomenon is not merely a curiosity but a biomechanical reality with implications for athletes, physical therapists, and anyone with hypermobility. The primary muscle involved in passive external rotation of the arm is the posterior capsule of the shoulder joint, which, when lax, allows the humeral head to rotate outward with minimal resistance. This increased range of motion can be both a blessing and a curse, depending on the context.
Consider the case of a gymnast or swimmer, whose performance may benefit from the extended range of motion provided by hypermobile shoulders. However, this advantage comes with a trade-off: the risk of instability and injury. The posterior capsule, along with the ligaments and labrum, provides critical stability to the shoulder joint. When these structures are overly lax, the joint becomes more susceptible to dislocation or impingement. For instance, a study published in the *Journal of Shoulder and Elbow Surgery* found that hypermobile individuals were 2.5 times more likely to experience shoulder dislocations compared to their non-hypermobile counterparts.
To manage this condition effectively, it’s essential to strengthen the dynamic stabilizers of the shoulder, such as the rotator cuff muscles (supraspinatus, infraspinatus, teres minor, and subscapularis). These muscles act as a secondary restraint system, compensating for the laxity in the static structures. A targeted exercise regimen might include external rotation with a resistance band (3 sets of 12–15 repetitions, 2–3 times per week) and scapular stabilization exercises like wall slides or prone Y’s. Avoid aggressive stretching or activities that emphasize end-range external rotation, as these can exacerbate instability.
Comparatively, individuals without hypermobility typically exhibit a more restricted passive external rotation, often limited to 60–70 degrees. In contrast, hypermobile shoulders may achieve 80 degrees or more. This disparity highlights the importance of individualized assessment and intervention. For example, a physical therapist might use the Beighton Score (a hypermobility assessment tool) to gauge joint laxity and tailor a program accordingly. Early intervention is key, particularly for adolescents and young adults, as this age group is most at risk for hypermobility-related injuries.
In conclusion, while greater passive external rotation in hypermobile shoulders may seem advantageous, it demands careful management. By understanding the role of the posterior capsule and implementing targeted strengthening exercises, individuals can harness the benefits of their range of motion while minimizing the risks. Practical tips include avoiding overhead activities without proper warm-up, using supportive braces during high-risk sports, and incorporating proprioceptive training to enhance joint awareness. With the right approach, hypermobility can be a strength rather than a liability.
Effective Upper Arm Muscle Building: Tips and Exercises for Strength
You may want to see also
Explore related products






![]()
Rotator Cuff Balance: Imbalanced rotator cuff muscles affect passive external rotation
The rotator cuff, a quartet of muscles stabilizing the shoulder joint, plays a pivotal role in both active and passive arm movements. Among these, passive external rotation—the ability to allow the arm to rotate outward without active muscle engagement—is particularly sensitive to imbalances within this group. When the rotator cuff muscles are not evenly developed or functioning harmoniously, passive external rotation can become restricted, leading to discomfort, reduced range of motion, and increased injury risk.
Consider the interplay between the infraspinatus and subscapularis, two key players in external rotation. The infraspinatus, located on the posterior side of the scapula, is the primary external rotator. Conversely, the subscapularis, situated on the anterior side, acts as an internal rotator. When the subscapularis becomes overdeveloped or tight relative to the infraspinatus, it can limit passive external rotation. For instance, athletes in sports like swimming or baseball often exhibit this imbalance due to repetitive internal rotation movements, resulting in a noticeable asymmetry in shoulder mobility.
Addressing this imbalance requires targeted strengthening and stretching exercises. Incorporate external rotation exercises with resistance bands or light dumbbells (2–3 sets of 12–15 reps, 3 times per week) to build infraspinatus strength. Simultaneously, perform subscapularis stretches, such as the sleeper stretch, holding for 30–60 seconds per side daily. For older adults (ages 50+), start with bodyweight or minimal resistance to avoid strain, gradually increasing intensity as strength improves.
A cautionary note: overcorrecting one muscle group can lead to new imbalances. Always pair strengthening exercises with mobility work for both internal and external rotators. For example, follow infraspinatus strengthening with a cross-body stretch for the subscapularis. Additionally, monitor progress through periodic range-of-motion assessments, such as measuring passive external rotation with a goniometer, to ensure balanced improvement.
In conclusion, restoring rotator cuff balance is essential for optimal passive external rotation. By understanding the specific roles of muscles like the infraspinatus and subscapularis, and implementing targeted exercises with mindful progression, individuals can enhance shoulder function and prevent long-term issues. Consistency and balance are key—whether you’re an athlete, desk worker, or senior aiming to maintain mobility.
Understanding Your Arm Muscles: Anatomy, Function, and Strengthening Tips
You may want to see also
Frequently asked questions
The passive external rotation of the arm is primarily facilitated by the joint capsule and ligaments of the shoulder, particularly the inferior glenohumeral ligament, rather than a specific muscle.
While passive external rotation is mainly due to ligamentous structures, the deltoid and rotator cuff muscles (especially the infraspinatus and teres minor) can contribute to maintaining the position when relaxed.
The joint capsule, especially the inferior glenohumeral ligament, provides stability and resistance to movement, allowing the arm to passively externally rotate when relaxed or under external force.
Passive external rotation is more about flexibility and joint mobility than muscle strength. Stretching exercises targeting the shoulder capsule and ligaments, such as cross-body arm stretches, can enhance this range of motion.
Conditions like adhesive capsulitis (frozen shoulder), rotator cuff injuries, or shoulder impingement can restrict passive external rotation due to stiffness, inflammation, or structural damage in the joint.