Impingement syndrome of the shoulder, often referred to as IR or internal rotation impingement, is primarily caused by the tightening or overuse of specific muscles surrounding the shoulder joint. The primary culprits include the rotator cuff muscles—supraspinatus, infraspinatus, teres minor, and subscapularis—which can become inflamed or irritated due to repetitive motions or poor posture. Additionally, the pectoralis major and latissimus dorsi muscles, which are involved in internal rotation and adduction, can contribute to impingement by pulling the humeral head forward, reducing the subacromial space and compressing the rotator cuff tendons. Understanding the role of these muscles is crucial for diagnosing and treating shoulder impingement effectively.
| Characteristics | Values |
|---|---|
| Muscles Involved | Subscapularis, Teres Minor, Infraspinatus, Supraspinatus, Deltoid, Pectoralis Major, Latissimus Dorsi, Teres Major, Coracobrachialis, Biceps Brachii, Triceps Brachii |
| Primary Cause of Impingement | Subscapularis and Infraspinatus (most common), Supraspinatus (second most common) |
| Mechanism of Injury | Repetitive overhead activities, trauma, muscle imbalances, poor posture, degenerative changes |
| Symptoms | Pain, weakness, limited range of motion, crepitus, night pain, difficulty with overhead activities |
| Diagnosis | Physical examination, imaging (X-ray, MRI, ultrasound), Neer and Hawkins-Kennedy impingement tests |
| Treatment | Rest, physical therapy, anti-inflammatory medications, corticosteroid injections, surgical intervention (in severe cases) |
| Prevention | Strengthening rotator cuff muscles, maintaining proper posture, avoiding repetitive overhead activities, gradual progression in exercise intensity |
| Associated Conditions | Rotator cuff tendinitis, bursitis, labral tears, AC joint arthritis |
| Risk Factors | Age, occupation (e.g., painters, swimmers), sports participation (e.g., baseball, tennis), genetic predisposition |
| Prognosis | Generally good with early intervention; chronic cases may require prolonged treatment or surgery |
Explore related products






What You'll Learn
- Rotator cuff muscles: Supraspinatus, infraspinatus, teres minor, subscapularis
- Biceps tendon: Long head involvement in shoulder impingement
- Deltoid muscle: Anterior fibers contribute to anterior shoulder pain
- Pectoralis major: Tightness causes internal rotation, impingement risk
- Scapular stabilizers: Weakness in serratus anterior, trapezius leads to dysfunction
![]()
Rotator cuff muscles: Supraspinatus, infraspinatus, teres minor, subscapularis
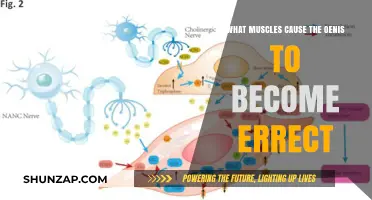
The rotator cuff is a group of four muscles that play a crucial role in shoulder stability and movement. These muscles—supraspinatus, infraspinatus, teres minor, and subscapularis—work together to maintain the humeral head within the glenoid fossa during shoulder motion. Injuries to these muscles are a common cause of shoulder pain and dysfunction, often referred to as "impingement" or "rotator cuff pathology." Understanding the function and location of each muscle is essential for identifying and addressing shoulder issues effectively.
The supraspinatus muscle originates in the supraspinous fossa of the scapula and inserts on the greater tubercle of the humerus. Its primary function is to initiate abduction of the shoulder, lifting the arm away from the body. The supraspinatus is frequently involved in rotator cuff injuries due to its vulnerable position beneath the acromion, where it can become impinged during overhead activities. Strengthening this muscle through exercises like external rotation with a resistance band or prone horizontal abduction can help prevent and rehabilitate injuries.
The infraspinatus and teres minor muscles are responsible for external rotation of the shoulder, a critical movement for activities like throwing or reaching behind the back. The infraspinatus originates in the infraspinous fossa of the scapula, while the teres minor originates on the lateral border of the scapula. Both insert on the greater tubercle of the humerus. These muscles are often injured in athletes or individuals who perform repetitive overhead motions. Strengthening exercises such as external rotation with a dumbbell or resistance band can target these muscles effectively.
The subscapularis is the largest and strongest rotator cuff muscle, originating on the subscapular fossa of the scapula and inserting on the lesser tubercle of the humerus. Its primary function is internal rotation of the shoulder, which is essential for activities like throwing a ball or lifting objects. The subscapularis also provides anterior stability to the shoulder joint. Injuries to this muscle are less common but can occur, particularly in individuals with prolonged shoulder instability. Exercises like internal rotation with a resistance band or wall push-ups can help strengthen the subscapularis.
In summary, the rotator cuff muscles—supraspinatus, infraspinatus, teres minor, and subscapularis—are vital for shoulder function and stability. Injuries to these muscles often result from overuse, trauma, or degenerative changes, leading to pain, weakness, and limited range of motion. Targeted strengthening and stretching exercises can prevent and rehabilitate rotator cuff injuries, emphasizing the importance of maintaining balance and coordination among these muscles. Proper understanding and care of the rotator cuff are key to preserving shoulder health and functionality.
Foot Muscle Cramps: Understanding the Root Cause
You may want to see also
Explore related products






![]()
Biceps tendon: Long head involvement in shoulder impingement
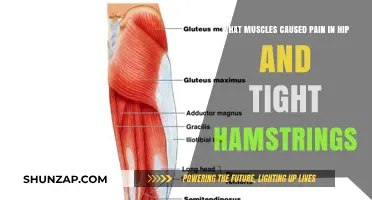
The biceps tendon, specifically the long head, plays a significant role in shoulder impingement syndrome, a common cause of shoulder pain and dysfunction. Shoulder impingement occurs when the rotator cuff tendons and/or the long head of the biceps tendon become compressed or irritated within the narrow subacromial space, leading to inflammation and pain. The long head of the biceps tendon is particularly vulnerable due to its unique anatomical position and function. It originates from the supraglenoid tubercle of the scapula, runs through the bicipital groove, and passes beneath the transverse humeral ligament within the subacromial space before attaching to the biceps muscle belly. This course makes it susceptible to friction and impingement, especially during repetitive overhead activities or with age-related degenerative changes.
Anatomically, the long head of the biceps tendon is closely associated with the rotator cuff and the labrum, contributing to shoulder stability and function. However, its intra-articular and extra-articular components make it prone to irritation, particularly in the setting of poor biomechanics or structural abnormalities. When the shoulder is in abduction or flexion, the long head of the biceps tendon moves anteriorly and superiorly, increasing the risk of impingement against the coracoacromial arch. Over time, this can lead to tendon inflammation (tendinitis) or degeneration (tendinosis), exacerbating impingement symptoms. Additionally, conditions such as biceps tendon subluxation or instability within the bicipital groove can further contribute to irritation and pain.
Clinically, patients with long head biceps tendon involvement in shoulder impingement often present with anterior or anterosuperior shoulder pain, which may radiate to the biceps muscle. Pain is typically exacerbated by activities requiring shoulder flexion, abduction, or rotation, such as lifting objects or reaching overhead. Specific provocative tests, like the Speed's test or Yergason's test, can help isolate biceps tendon pathology. Imaging studies, including ultrasound or MRI, may reveal tendon thickening, inflammation, or partial tears, confirming the diagnosis. Addressing biceps tendon involvement is crucial, as untreated pathology can lead to chronic impingement, rotator cuff tears, or even biceps tendon rupture.
Management of biceps tendon involvement in shoulder impingement focuses on reducing inflammation, restoring normal biomechanics, and strengthening the surrounding musculature. Initial treatment is typically conservative, involving activity modification, nonsteroidal anti-inflammatory drugs (NSAIDs), and physical therapy. Therapeutic exercises aim to improve scapular stability, rotator cuff strength, and biceps tendon mobility while avoiding aggravating movements. In cases of persistent symptoms, corticosteroid injections may be considered to alleviate pain and inflammation, although their use should be judicious to avoid tendon weakening. Surgical intervention, such as biceps tenodesis or tenotomy, may be warranted for refractory cases or significant tendon pathology, particularly when conservative measures fail to provide relief.
In summary, the long head of the biceps tendon is a critical structure in shoulder impingement syndrome due to its anatomical course and functional demands. Its involvement can lead to significant pain and dysfunction, particularly during overhead activities. Understanding the role of the biceps tendon in impingement is essential for accurate diagnosis and targeted treatment. A comprehensive approach, combining conservative management and, if necessary, surgical intervention, can effectively address biceps tendon pathology and improve patient outcomes in shoulder impingement syndrome.
Lipitor and Muscle Pain: What's the Link?
You may want to see also
Explore related products






![]()
Deltoid muscle: Anterior fibers contribute to anterior shoulder pain
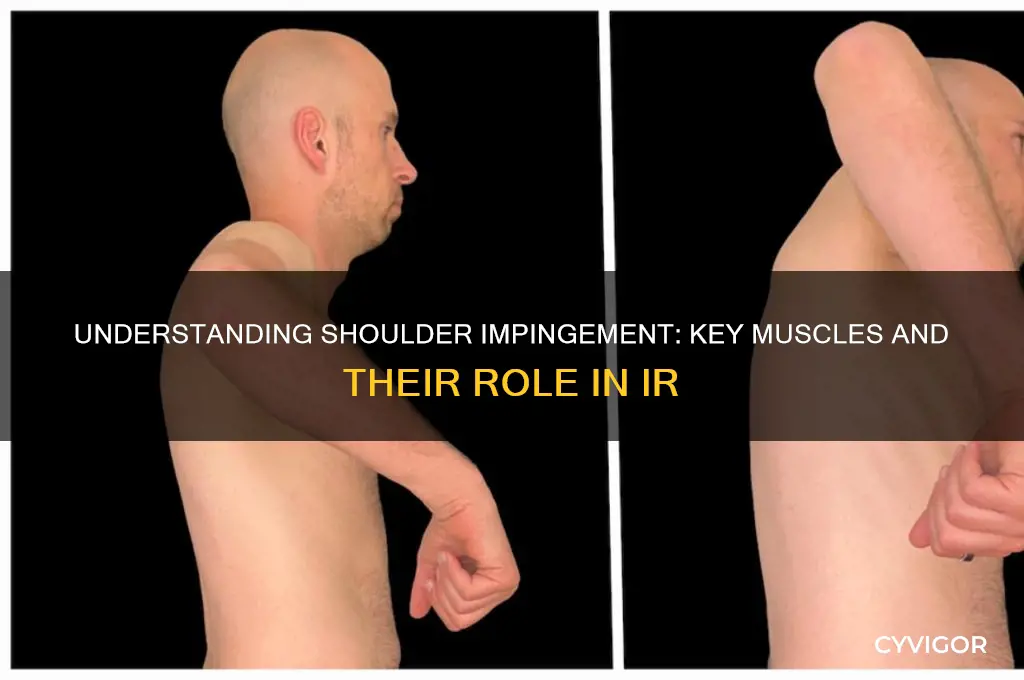
The deltoid muscle, a key contributor to shoulder movement and stability, is often implicated in shoulder pain, particularly when its anterior fibers are involved. The deltoid is a large, triangular muscle that covers the shoulder joint and is divided into three sets of fibers: anterior (front), lateral (side), and posterior (rear). The anterior fibers of the deltoid originate on the clavicle (collarbone) and insert on the humerus (upper arm bone). Their primary function is to assist in shoulder flexion (lifting the arm forward) and internal rotation. However, when these fibers become strained, overused, or inflamed, they can contribute significantly to anterior shoulder pain.
Anterior shoulder pain associated with the deltoid muscle often arises from repetitive overhead activities, such as throwing, swimming, or weightlifting. These movements place excessive stress on the anterior deltoid fibers, leading to microtears, tendinitis, or muscle strain. Additionally, poor posture, such as rounded shoulders or a forward head position, can chronically tighten the anterior deltoid, causing it to become a source of pain and discomfort. Individuals experiencing this type of pain typically report a dull ache in the front of the shoulder, which may worsen with movement or palpation of the muscle.
To address anterior shoulder pain caused by the deltoid muscle, it is essential to focus on both strengthening and stretching the affected fibers. Strengthening exercises should target the deltoid while also engaging the rotator cuff muscles to improve overall shoulder stability. Examples include resisted shoulder flexion with bands or weights and isometric shoulder presses. Stretching the anterior deltoid is equally important to alleviate tightness and restore proper muscle length. A simple stretch involves crossing the arm across the chest and gently pulling it toward the opposite shoulder until a mild stretch is felt in the front of the shoulder.
Incorporating corrective exercises to address postural imbalances can also help prevent recurrent anterior deltoid issues. For instance, exercises that strengthen the upper back and rear shoulder muscles, such as rows and external rotations, can counteract the effects of poor posture. Foam rolling or self-myofascial release techniques can be applied to the deltoid to relieve tension and promote healing. It is crucial to perform these exercises with proper form and avoid overloading the muscle, as this can exacerbate the pain.
Finally, rest and activity modification are vital components of managing anterior shoulder pain related to the deltoid. Avoiding activities that aggravate the pain, such as repetitive overhead motions, allows the muscle to heal. Applying ice to the affected area can reduce inflammation and numb the pain, while heat therapy may be beneficial once the acute phase has passed to increase blood flow and flexibility. If pain persists or worsens despite these measures, consulting a healthcare professional is recommended to rule out more serious conditions, such as a rotator cuff tear or labral injury, and to receive a tailored treatment plan.
Horse Chestnut: A Muscle Weakness Trigger?
You may want to see also
Explore related products






![]()
Pectoralis major: Tightness causes internal rotation, impingement risk
The pectoralis major, a large muscle spanning the chest, plays a significant role in shoulder mechanics. When this muscle becomes tight, it can contribute to internal rotation of the shoulder joint, a movement where the arm rotates inward towards the body. This tightness is often a result of repetitive activities or poor posture, such as prolonged desk work or excessive bench pressing without proper stretching. Over time, the pectoralis major can shorten, pulling the shoulder into a more internally rotated position, which may lead to various shoulder issues.
Tightness in the pectoralis major can directly impact the shoulder's range of motion and stability. As the muscle tightens, it restricts the outward rotation of the shoulder, causing an imbalance in the joint's natural movement. This imbalance can lead to a condition known as impingement, where the rotator cuff tendons become compressed or irritated, resulting in pain and potential injury. Impingement syndrome is a common issue for athletes and individuals with occupations requiring repetitive overhead movements.
To address this issue, stretching and strengthening exercises targeting the pectoralis major and surrounding muscles are essential. Stretching the tight pectoralis major muscle can help restore the shoulder's natural range of motion and alleviate internal rotation. Simple stretches like the corner stretch or using a foam roller can be effective. Additionally, strengthening the external rotators of the shoulder, such as the infraspinatus and teres minor muscles, can help counteract the internal rotation caused by pectoralis major tightness.
It is crucial to maintain a balanced exercise routine to prevent and manage this condition. Individuals should focus on exercises that promote shoulder stability and mobility, ensuring that the pectoralis major is not overworked in relation to other shoulder muscles. For instance, incorporating rows and external rotation exercises can help maintain muscle balance. By addressing pectoralis major tightness and its impact on internal rotation, individuals can reduce the risk of shoulder impingement and maintain optimal shoulder health.
In summary, the pectoralis major's tightness can significantly contribute to internal rotation of the shoulder, increasing the likelihood of impingement syndrome. Understanding this relationship is vital for athletes, fitness enthusiasts, and individuals with occupations that may predispose them to shoulder issues. Through targeted stretching and strengthening exercises, it is possible to manage and prevent these problems, ensuring the shoulder joint remains healthy and functional. This knowledge empowers individuals to take proactive measures in their fitness and daily routines.
Flagyl and Muscle Pain: What's the Link?
You may want to see also
Explore related products






![]()
Scapular stabilizers: Weakness in serratus anterior, trapezius leads to dysfunction
The scapular stabilizers play a crucial role in maintaining proper shoulder mechanics and preventing injuries. Among these, the serratus anterior and trapezius muscles are particularly vital. The serratus anterior, often referred to as the "big swing muscle," is responsible for protracting, rotating, and stabilizing the scapula against the rib cage. It ensures the scapula moves smoothly during arm elevation, preventing winging of the shoulder blade. The trapezius, on the other hand, is a large muscle that spans the upper back, shoulders, and neck, aiding in scapular elevation, depression, upward rotation, and retraction. Weakness in either of these muscles can disrupt scapular stability, leading to dysfunctional shoulder movement and increased risk of injury.
When the serratus anterior is weak, the scapula may wing outward, causing improper alignment and movement during overhead activities. This dysfunction is often observed in athletes or individuals who perform repetitive overhead motions, such as swimmers, baseball players, or weightlifters. Winging of the scapula reduces the efficiency of shoulder movement and places excessive stress on other structures, such as the rotator cuff and labrum. Over time, this can lead to impingement, rotator cuff tears, or even instability in the shoulder joint. Strengthening the serratus anterior through exercises like scapular push-ups, wall slides, and banded serratus punches is essential to restore proper function.
Similarly, weakness in the trapezius muscle, particularly the middle and lower fibers, can impair scapular upward rotation and retraction. This deficiency often results in a depressed or protracted scapula, limiting the range of motion during arm elevation. Individuals with trapezius weakness may experience difficulty reaching overhead or maintaining proper posture, which can contribute to shoulder pain and dysfunction. The trapezius also plays a key role in counterbalancing the action of the pectoralis minor, preventing the scapula from becoming excessively protracted. Strengthening the trapezius through exercises like face pulls, rows, and shrugs can help address this imbalance and improve scapular stability.
The interplay between the serratus anterior and trapezius is critical for optimal shoulder function. Dysfunction in one muscle often affects the other, creating a cycle of instability and compensatory movements. For example, a weak serratus anterior may lead to over-reliance on the trapezius, causing it to fatigue and weaken over time. Conversely, trapezius weakness can place excessive demand on the serratus anterior, leading to similar issues. Addressing both muscles simultaneously through targeted strengthening and corrective exercises is essential for restoring balance and preventing further injury.
Incorporating scapular stabilization exercises into a rehabilitation or preventive program is key to addressing weakness in the serratus anterior and trapezius. Exercises such as scapular retractions, YTWs, and prone cobras can help activate and strengthen these muscles while promoting proper movement patterns. Additionally, focusing on posture and avoiding prolonged positions that strain the scapular stabilizers, such as slouching or hunching, is crucial. By prioritizing the health of these muscles, individuals can reduce their risk of shoulder dysfunction and maintain long-term shoulder health.
Understanding Muscle Fatigue and Pain During Exercise: Causes Explained
You may want to see also
Frequently asked questions
The rotator cuff muscles (supraspinatus, infraspinatus, teres minor, and subscapularis) are most commonly involved in shoulder impingement. The supraspinatus is particularly susceptible due to its location beneath the acromion.
The subscapularis is the primary internal rotator of the shoulder. Tightness or weakness in this muscle can lead to imbalances, causing excessive internal rotation and contributing to impingement or instability.
Yes, tightness in the pectoralis major can pull the shoulder forward, promoting excessive internal rotation. This alters shoulder mechanics, increasing the risk of impingement and other overuse injuries.