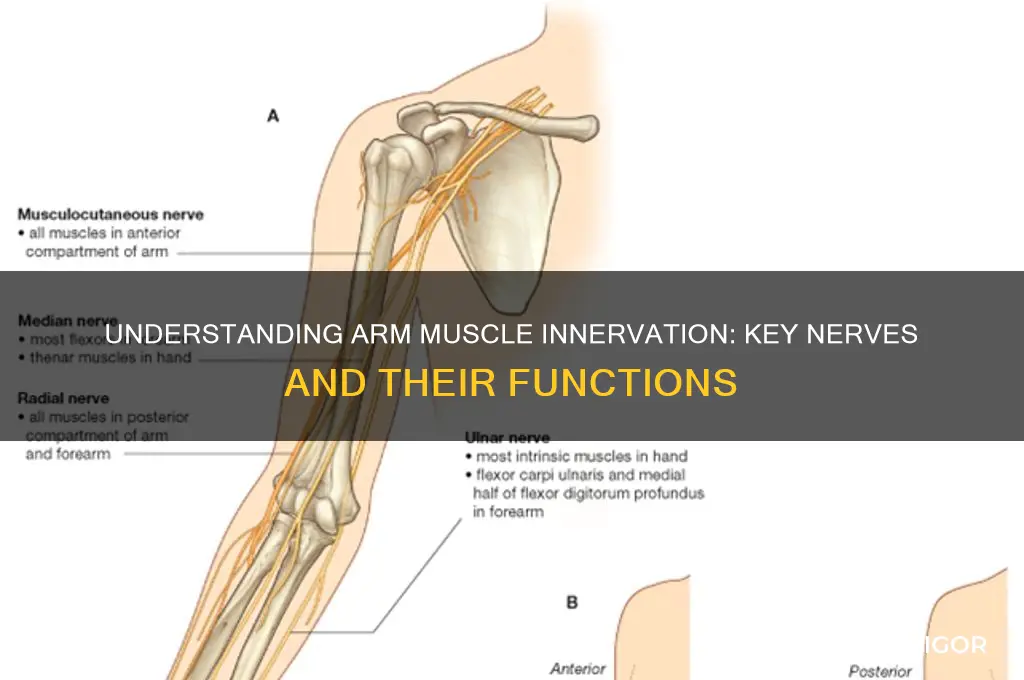
The arm muscles are innervated by a complex network of nerves that originate from the brachial plexus, a bundle of nerve fibers formed by the lower cervical and upper thoracic nerve roots (C5-T1). These nerves primarily include the musculocutaneous nerve, which supplies muscles in the anterior compartment of the arm such as the biceps brachii, brachialis, and coracobrachialis; the radial nerve, responsible for innervating the posterior compartment muscles like the triceps brachii, anconeus, and extensor muscles of the forearm; and the axillary nerve, which innervates the deltoid and teres minor muscles in the shoulder region. Understanding the specific innervation of these nerves is crucial for diagnosing and treating conditions such as nerve injuries, muscle weakness, or sensory deficits in the arm.
Explore related products






What You'll Learn
- Musculocutaneous Nerve: Innervates flexor muscles of arm, forearm, and lateral forearm skin
- Radial Nerve: Supplies triceps, extensor muscles, and posterior arm/forearm skin
- Median Nerve: Controls forearm flexors, thenar muscles, and palmar skin sensation
- Ulnar Nerve: Innervates intrinsic hand muscles, medial forearm flexors, and ulnar hand skin
- Axillary Nerve: Supplies deltoid, teres minor, and shoulder joint sensory fibers
![]()
Musculocutaneous Nerve: Innervates flexor muscles of arm, forearm, and lateral forearm skin
The musculocutaneous nerve is a critical player in the intricate network of nerves that control arm movement and sensation. Originating from the lateral cord of the brachial plexus, it travels through the arm, supplying motor innervation to key flexor muscles and sensory innervation to the lateral forearm skin. This nerve’s pathway and function highlight its role in both voluntary movement and tactile perception, making it essential for daily activities like lifting, gripping, and feeling objects.
Consider the musculocutaneous nerve as the conductor of a symphony, orchestrating the contraction of the biceps brachii, coracobrachialis, and brachialis muscles. These muscles are responsible for flexing the arm at the elbow and shoulder, actions fundamental to tasks ranging from carrying groceries to throwing a ball. Without proper innervation from this nerve, even simple movements could become labored or impossible. For instance, damage to the musculocutaneous nerve might result in a weakened biceps brachii, impairing the ability to lift objects or bend the elbow effectively.
Sensory innervation is another vital function of the musculocutaneous nerve. It provides tactile sensation to the lateral forearm skin, allowing you to perceive textures, temperatures, and pressure. This sensory feedback is crucial for fine motor skills, such as buttoning a shirt or typing. To test its function, lightly touch the lateral side of your forearm and note the immediate sensation—this is the musculocutaneous nerve at work. If sensation is diminished, it could indicate nerve compression or injury, warranting medical evaluation.
Practical tips for maintaining the health of the musculocutaneous nerve include avoiding prolonged pressure on the arm, such as leaning on elbows for extended periods, which can compress the nerve. Incorporating nerve-gliding exercises into your routine can also enhance flexibility and reduce the risk of injury. For example, gently rotating your forearm while extending and flexing your elbow helps mobilize the nerve within its pathway. If you experience persistent weakness, numbness, or pain in the arm or forearm, consult a healthcare professional for a thorough assessment, as early intervention can prevent long-term complications.
In summary, the musculocutaneous nerve is indispensable for both motor and sensory functions in the arm and forearm. Understanding its role and taking proactive steps to protect it can safeguard your ability to perform everyday activities with ease. Whether through mindful ergonomics or targeted exercises, prioritizing nerve health ensures continued functionality and comfort in your upper extremities.
Sculpt & Define: Contouring Arm Muscles with Makeup Techniques
You may want to see also
Explore related products






![]()
Radial Nerve: Supplies triceps, extensor muscles, and posterior arm/forearm skin
The radial nerve, a powerhouse in the upper limb, plays a pivotal role in arm functionality. Originating from the brachial plexus, it courses down the arm, supplying critical muscles and sensory areas. Its primary responsibility lies in innervating the triceps brachii, the muscle group essential for elbow extension. This nerve also extends its influence to the extensor muscles of the forearm, enabling movements like wrist and finger extension. Beyond motor control, the radial nerve provides sensory innervation to the posterior aspect of the arm and forearm, ensuring tactile feedback from these regions.
Consider the practical implications of radial nerve function in daily activities. Whether lifting a cup or typing on a keyboard, the coordinated action of triceps and forearm extensors is indispensable. Damage to this nerve, often referred to as radial nerve palsy, can result in a characteristic "wrist drop" due to weakened extensor muscles. Rehabilitation for such injuries typically involves targeted exercises to restore strength and mobility, emphasizing gradual progression to avoid overexertion. For instance, starting with gentle wrist extension exercises using light resistance bands can help rebuild muscle control without straining the healing nerve.
From an anatomical perspective, the radial nerve’s pathway highlights its vulnerability. As it winds around the humerus, it passes through a narrow space known as the spiral groove, where it is susceptible to compression or injury. Athletes and manual laborers, who frequently engage in repetitive arm movements, are particularly at risk. Preventive measures, such as ergonomic adjustments and regular stretching, can mitigate this risk. For example, incorporating forearm stretches into a post-workout routine can alleviate tension around the nerve, reducing the likelihood of impingement.
In clinical settings, assessing radial nerve function is straightforward yet crucial. A simple test involves asking the patient to extend their elbow against resistance or lift their wrist against gravity. Sensory evaluation can be performed by testing light touch or pinprick sensation along the posterior arm and forearm. Early detection of deficits allows for timely intervention, which is vital for optimal recovery. For patients with radial nerve palsy, combining physical therapy with modalities like ultrasound or electrical stimulation can enhance healing, though the specific approach should be tailored to the individual’s condition and tolerance.
Understanding the radial nerve’s role underscores its significance in both anatomy and everyday life. By recognizing its functions and vulnerabilities, individuals can take proactive steps to protect this vital structure. Whether through preventive measures, targeted exercises, or informed clinical assessments, safeguarding the radial nerve ensures continued arm functionality and quality of life. Its unique contributions to movement and sensation make it a cornerstone of upper limb physiology, deserving of attention and care.
Revitalize Aging Arms: Effective Muscle Toning Tips for Older Men
You may want to see also
Explore related products





![]()
Median Nerve: Controls forearm flexors, thenar muscles, and palmar skin sensation
The median nerve, a key player in upper limb function, originates from the brachial plexus and travels down the arm, passing through the cubital fossa and into the forearm. It is responsible for innervating some of the most crucial muscles involved in fine motor skills and grip strength. Understanding its role is essential for anyone from medical professionals diagnosing nerve injuries to fitness enthusiasts aiming to optimize arm workouts.
Consider the practical implications of median nerve function in daily activities. When you grip a coffee cup, flex your wrist to check your watch, or use your thumb to swipe on a smartphone, the median nerve is at work. It innervates the forearm flexors, such as the flexor carpi radialis and palmaris longus, enabling precise movements. Additionally, it controls the thenar muscles—those small but mighty muscles at the base of the thumb—which are vital for tasks requiring dexterity, like buttoning a shirt or holding a pen.
A median nerve injury, such as carpal tunnel syndrome, can severely impair these functions. Symptoms often include numbness or tingling in the palmar skin, weakness in thumb abduction, and difficulty performing tasks requiring fine motor skills. Early intervention is critical; treatments range from conservative measures like wrist splinting and corticosteroid injections to surgical decompression in severe cases. For prevention, ergonomic adjustments in workspaces and regular stretching exercises can reduce strain on the median nerve.
Comparing the median nerve to other nerves in the arm highlights its unique role. While the ulnar nerve innervates the intrinsic hand muscles and the radial nerve controls the forearm extensors, the median nerve bridges both movement and sensation in the forearm and hand. This duality makes it a critical focus in both clinical assessments and rehabilitative therapies. For instance, a patient with median nerve damage might regain strength through targeted exercises like thumb opposition drills and wrist flexion stretches, paired with sensory re-education techniques to restore palmar skin sensation.
Incorporating median nerve health into fitness routines can enhance performance and prevent injury. Athletes and weightlifters should include exercises that strengthen the forearm flexors and thenar muscles, such as wrist curls and thumb resistance bands. However, caution is advised: excessive repetitive motions, like prolonged typing or heavy gripping, can compress the nerve at the wrist. Balancing strength training with flexibility exercises, like nerve gliding techniques, ensures optimal function and longevity.
By recognizing the median nerve’s specific contributions to arm and hand function, individuals can better protect and enhance their upper limb capabilities. Whether through injury prevention, targeted rehabilitation, or mindful exercise, understanding this nerve’s role empowers proactive care and informed decision-making.
Strengthen Your Shoulders: Muscles Engaged by Holding Arms Out
You may want to see also
Explore related products






![]()
Ulnar Nerve: Innervates intrinsic hand muscles, medial forearm flexors, and ulnar hand skin
The ulnar nerve, often referred to as the "musician's nerve," plays a pivotal role in hand function, particularly in fine motor skills and grip strength. Originating from the brachial plexus, it travels down the arm, passing through the cubital tunnel at the elbow before terminating in the hand. This nerve is responsible for innervating the intrinsic hand muscles, which are essential for movements like gripping, pinching, and manipulating small objects. Without proper ulnar nerve function, tasks requiring dexterity—such as playing an instrument, typing, or buttoning a shirt—become significantly impaired.
Consider the anatomy: the ulnar nerve supplies the medial forearm flexors, including the flexor carpi ulnaris and the ulnar half of the flexor digitorum profundus. These muscles are crucial for wrist flexion and finger bending, enabling actions like holding a cup or lifting weights. Additionally, the nerve provides sensory innervation to the ulnar side of the hand, including the little finger and the medial half of the ring finger. Damage to this nerve, such as from compression at the elbow (cubital tunnel syndrome), can result in numbness, tingling, or weakness in these areas, often referred to as "ulnar claw hand" due to the characteristic claw-like deformity of the fingers.
To protect ulnar nerve health, ergonomic adjustments are key. Avoid prolonged pressure on the elbow, such as leaning on it for extended periods, as this can compress the nerve. When sleeping, use a towel or splint to keep the elbow straight, reducing the risk of irritation. For musicians or athletes, regular hand and forearm stretches can alleviate tension around the nerve. If symptoms like persistent numbness or weakness arise, consult a healthcare professional promptly. Early intervention, such as physical therapy or, in severe cases, surgical decompression, can prevent long-term damage.
Comparatively, the ulnar nerve’s role contrasts with that of the median and radial nerves, which innervate different muscle groups and sensory areas. While the median nerve controls the thumb and radial side of the hand, the ulnar nerve’s focus on intrinsic muscles and medial flexors highlights its unique contribution to hand function. Understanding this distinction is crucial for diagnosing nerve-related issues accurately. For instance, carpal tunnel syndrome affects the median nerve, whereas ulnar nerve compression manifests differently, emphasizing the need for targeted treatment approaches.
In practical terms, strengthening exercises can support ulnar nerve function. Squeeze a stress ball or perform finger resistance exercises using therapy putty to enhance intrinsic muscle strength. For sensory issues, contrast baths—alternating warm and cold water immersion—can improve circulation and nerve responsiveness. Always start with gentle movements and gradually increase intensity to avoid strain. By prioritizing ulnar nerve health, individuals can maintain the precision and strength required for daily activities and specialized skills alike.
Understanding the Biceps Brachii: Arm Flexion and Medial Rotation Explained
You may want to see also
Explore related products






![]()
Axillary Nerve: Supplies deltoid, teres minor, and shoulder joint sensory fibers
The axillary nerve, a branch of the brachial plexus, plays a crucial, yet often underappreciated, role in upper limb function. Originating from the C5 and C6 nerve roots, it courses through the quadrilateral space, a narrow passage bounded by the humerus, teres minor, teres major, and long head of the triceps. This anatomical pathway is vital for understanding its function and vulnerability to injury.
Example: A common scenario involves a patient presenting with shoulder weakness and atrophy of the deltoid muscle after a dislocation. This is often due to axillary nerve damage, highlighting its critical role in shoulder abduction and stability.
Analysis: The axillary nerve’s primary motor functions are to innervate the deltoid and teres minor muscles. The deltoid, responsible for shoulder abduction, is particularly dependent on this nerve. Teres minor, part of the rotator cuff, assists in external rotation and stabilizes the humeral head. Sensory fibers from the axillary nerve supply the skin over the lateral shoulder, a region known as the "regimental badge" area. This dual role—motor and sensory—makes the axillary nerve indispensable for both movement and proprioception in the shoulder.
Takeaway: Clinicians and therapists must prioritize assessing the axillary nerve in patients with shoulder injuries. A thorough examination includes testing deltoid strength (abduction against resistance) and teres minor function (external rotation with the arm abducted). Sensory deficits in the lateral shoulder should also raise suspicion of axillary nerve involvement. Early diagnosis can prevent long-term complications, such as deltoid atrophy or chronic instability.
Steps for Rehabilitation: For patients with axillary nerve injuries, rehabilitation focuses on preserving muscle function and preventing contractures. Initial treatment includes gentle range-of-motion exercises for the shoulder, avoiding excessive abduction or external rotation. Electrical stimulation of the deltoid and teres minor can help maintain muscle tone. As healing progresses, progressive resistance exercises are introduced, starting with isometrics and advancing to dynamic movements. Caution: Overloading the shoulder during recovery can exacerbate nerve damage, so gradual progression is key.
Practical Tips: Athletes or individuals with overhead activities (e.g., swimmers, painters) are at higher risk for axillary nerve injuries. To prevent damage, incorporate shoulder-strengthening exercises targeting the rotator cuff and deltoid. Stretching the posterior capsule can also reduce impingement risk. For those recovering from injury, consider using a sling to protect the shoulder during sleep, as nocturnal movements can strain the nerve. Regular follow-ups with a neurologist or orthopedist are essential to monitor nerve regeneration and adjust treatment plans accordingly.
Effective Remedies to Relieve Upper Arm and Shoulder Muscle Soreness
You may want to see also
Frequently asked questions
The muscles of the upper arm are primarily innervated by the musculocutaneous nerve (for the coracobrachialis, biceps brachii, and brachialis) and the axillary nerve (for the deltoid and teres minor).
The radial nerve innervates the triceps muscle, which is responsible for extending the elbow.
The forearm muscles are innervated by three main nerves: the median nerve, ulnar nerve, and radial nerve. The radial nerve supplies the extensor muscles, the median nerve supplies some flexors and pronators, and the ulnar nerve supplies other flexors and intrinsic hand muscles.
Yes, the brachial plexus is a network of nerves formed by the lower cervical and upper thoracic nerve roots (C5-T1). It gives rise to the major nerves (musculocutaneous, radial, axillary, median, and ulnar) that innervate the arm and forearm muscles.


![[360° Full Compression] Copper Arm Sleeves for Men & Women, [Ultra Breathable] Arm Brace for Forearm, Bicep, Triceps, Tennis Elbow, Basketball, Golf, Arthritis, Tendonitis, Bursitis](https://m.media-amazon.com/images/I/61YJAVr6e5L._AC_UL320_.jpg)