Smooth muscle contraction is primarily regulated by calcium-dependent mechanisms, but emerging research highlights the involvement of alternative signaling pathways. Beyond the classic calcium-calmodulin-myosin light chain kinase (MLCK) pathway, other mechanisms such as Rho-kinase activation, nitric oxide (NO) signaling, and G protein-coupled receptor (GPCR) pathways play significant roles. Rho-kinase, for instance, directly phosphorylates myosin light chains, enhancing contraction independently of calcium. Similarly, NO-mediated signaling can relax smooth muscle by activating soluble guanylate cyclase and increasing cyclic GMP levels, while dysregulation of this pathway may contribute to contraction. Additionally, GPCRs can modulate smooth muscle tone through second messengers like cyclic AMP or IP3, influencing calcium release and contractile activity. Understanding these diverse signaling mechanisms provides insights into the complex regulation of smooth muscle function and potential therapeutic targets for disorders involving abnormal contraction.
| Characteristics | Values |
|---|---|
| Signaling Mechanism | Rho-kinase pathway |
| Activation Trigger | Increase in intracellular calcium or G protein-coupled receptor (GPCR) activation |
| Key Enzyme | Rho-associated protein kinase (ROCK) |
| Effect on Smooth Muscle | Phosphorylation of myosin light chain phosphatase (MLCP), leading to contraction |
| Calcium Dependency | Can operate independently of calcium but is enhanced by calcium-dependent pathways |
| Role in Tone Regulation | Maintains basal tone in blood vessels and other smooth muscles |
| Inhibitors | ROCK inhibitors (e.g., Y-27632, Fasudil) |
| Clinical Relevance | Targeted in treatments for hypertension, asthma, and erectile dysfunction |
| Alternative Pathway | Acts parallel to the calcium-calmodulin-MLC kinase pathway |
| Cellular Localization | Primarily in the cytosol and associated with actin filaments |
| Downstream Effects | Increased actin-myosin interaction and sustained muscle contraction |
Explore related products





What You'll Learn
![]()
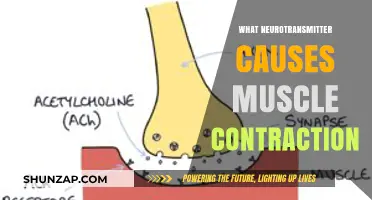
G Protein-Coupled Receptors (GPCRs)
The process of GPCR-mediated smooth muscle contraction involves several key steps. Firstly, the binding of a ligand, such as a hormone or neurotransmitter, to the GPCR causes the exchange of GDP for GTP on the G protein's α-subunit. This activates the G protein, allowing it to dissociate from the receptor and interact with downstream effectors. One of the primary effectors of G protein signaling in smooth muscle is the enzyme phospholipase C (PLC). Activation of PLC leads to the hydrolysis of phosphatidylinositol 4,5-bisphosphate (PIP2) into inositol 1,4,5-trisphosphate (IP3) and diacylglycerol (DAG). IP3 then binds to IP3 receptors on the sarcoplasmic reticulum, causing the release of calcium ions (Ca2+) into the cytoplasm.
The increase in cytoplasmic Ca2+ concentration is a crucial step in smooth muscle contraction. Ca2+ binds to calmodulin, forming a Ca2+/calmodulin complex that activates myosin light-chain kinase (MLCK). MLCK phosphorylates the myosin light chains, allowing them to interact with actin filaments and generate force. Additionally, DAG, another product of PLC activation, can activate protein kinase C (PKC), which further enhances the contractile response by phosphorylating various proteins involved in the contractile machinery. This coordinated activation of MLCK and PKC ensures a robust and sustained smooth muscle contraction.
GPCRs can couple to different types of G proteins, leading to diverse signaling outcomes. For example, Gq-coupled receptors, such as those activated by angiotensin II or endothelin-1, primarily activate the PLC pathway, resulting in Ca2+-mediated contraction. In contrast, Gi-coupled receptors, such as those activated by certain prostaglandins or adenosine, can inhibit adenylate cyclase, reducing cyclic AMP (cAMP) levels and indirectly promoting contraction by removing the relaxing effects of cAMP-dependent pathways. This versatility allows GPCRs to fine-tune smooth muscle tone in response to various physiological and pathophysiological stimuli.
Understanding the role of GPCRs in smooth muscle contraction has important clinical implications. Many therapeutic agents target GPCRs to modulate smooth muscle function in conditions such as hypertension, asthma, and gastrointestinal disorders. For instance, antagonists of Gq-coupled receptors like angiotensin II type 1 (AT1) receptors are used to treat hypertension by reducing vasoconstriction. Similarly, agonists of Gi-coupled receptors, such as certain prostaglandin analogs, can be used to promote smooth muscle relaxation in specific contexts. By targeting GPCRs, clinicians can effectively manage disorders involving abnormal smooth muscle tone, highlighting the central role of these receptors in both physiology and pharmacology.
Tonsillitis and Muscle Aches: What's the Connection?
You may want to see also
Explore related products






![]()
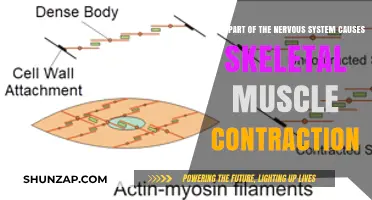
Tyrosine Kinase Receptors (RTKs)
In the context of smooth muscle contraction, RTKs such as the Platelet-Derived Growth Factor Receptor (PDGFR) and the Vascular Endothelial Growth Factor Receptor (VEGFR) are particularly significant. When activated, these receptors phosphorylate adaptor proteins like Shc and Grb2, which in turn activate Ras and subsequently the MAPK pathway. This signaling cascade leads to the phosphorylation of myosin light chain (MLC) through the activation of MLC kinase (MLCK), a critical step in smooth muscle contraction. Additionally, RTKs can modulate the activity of Rho kinase (ROCK), another key regulator of MLC phosphorylation, further enhancing contractile force.
Another important mechanism by which RTKs contribute to smooth muscle contraction involves the regulation of calcium sensitivity. RTK signaling can activate the phosphatidylinositol 3-kinase (PI3K)/Akt pathway, which influences the activity of calcium-sensitive proteins. For instance, Akt can phosphorylate and inhibit myosin phosphatase, leading to sustained MLC phosphorylation and prolonged contraction. Furthermore, RTKs can indirectly affect calcium influx by modulating the activity of ion channels and pumps, such as the L-type calcium channels and the plasma membrane Ca²⁺ ATPase (PMCA), thereby altering intracellular calcium levels and contractility.
RTKs also intersect with G protein-coupled receptor (GPCR) signaling pathways, which are traditionally associated with smooth muscle contraction. Cross-talk between RTKs and GPCRs can amplify contractile responses by converging on common downstream effectors, such as RhoA and ROCK. For example, activation of RTKs can enhance GPCR-mediated calcium mobilization and sensitization of the contractile machinery, creating a synergistic effect on smooth muscle tone. This interplay highlights the complexity and integration of signaling mechanisms in smooth muscle regulation.
In summary, Tyrosine Kinase Receptors (RTKs) are integral to smooth muscle contraction through their ability to activate multiple signaling pathways, including Ras/MAPK, PI3K/Akt, and RhoA/ROCK. By modulating MLC phosphorylation, calcium sensitivity, and intracellular calcium levels, RTKs provide a robust mechanism for regulating contractile responses. Their cross-talk with GPCRs further underscores their importance in orchestrating the intricate signaling networks that control smooth muscle function. Understanding these mechanisms not only advances our knowledge of smooth muscle physiology but also opens avenues for therapeutic interventions in conditions involving dysregulated smooth muscle contraction.
Muscle Strain and Lightheadedness: Is There a Link?
You may want to see also
Explore related products





![]()
Cyclic Nucleotide Pathways
Smooth muscle contraction is a complex process regulated by various signaling mechanisms, and one of the key pathways involved is the Cyclic Nucleotide Pathway. This pathway primarily revolves around the second messengers cyclic adenosine monophosphate (cAMP) and cyclic guanosine monophosphate (cGMP), which play critical roles in modulating smooth muscle tone. The activation of these pathways often leads to relaxation of smooth muscle, but under certain conditions, they can also contribute to contraction, depending on the specific cellular context and downstream effectors.
The cAMP pathway is initiated when agonists such as adrenaline or beta-adrenergic receptor stimulators bind to G protein-coupled receptors (GPCRs) on the smooth muscle cell membrane. This binding activates Gs proteins, which stimulate adenylate cyclase to convert ATP into cAMP. cAMP then binds to protein kinase A (PKA), leading to its activation. PKA phosphorylates target proteins, including phospholamban, which increases calcium reuptake into the sarcoplasmic reticulum, thereby reducing cytoplasmic calcium levels and promoting muscle relaxation. However, in some tissues, PKA can also phosphorylate other proteins that indirectly enhance calcium sensitivity or modulate contractile machinery, potentially contributing to contraction under specific conditions.
The cGMP pathway operates similarly but is primarily associated with nitric oxide (NO) signaling. When NO is released from endothelial cells or produced within smooth muscle cells, it activates soluble guanylate cyclase (sGC), which converts GTP into cGMP. cGMP binds to protein kinase G (PKG), leading to its activation. PKG phosphorylates target proteins, including those involved in calcium handling, such as phospholamban and calcium channels. This reduces intracellular calcium levels, promoting relaxation. However, like cAMP, cGMP signaling can also intersect with pathways that modulate contractility, depending on the specific cellular environment and the presence of other signaling molecules.
Cross-talk between cAMP and cGMP pathways is another critical aspect of cyclic nucleotide signaling in smooth muscle. Phosphodiesterases (PDEs) regulate the levels of cAMP and cGMP by hydrolyzing them into inactive forms. Inhibitors of specific PDEs, such as PDE5 inhibitors (e.g., sildenafil), increase cGMP levels, enhancing relaxation. Conversely, PDE4 inhibitors elevate cAMP levels, which can also promote relaxation. However, the balance between these pathways can shift under different physiological or pathological conditions, potentially leading to contraction if calcium sensitivity or influx is altered.
In summary, Cyclic Nucleotide Pathways involving cAMP and cGMP are central to smooth muscle regulation, primarily promoting relaxation through their effects on calcium handling. However, their interplay with other signaling mechanisms, such as calcium-sensitizing proteins or contractile machinery, can lead to contraction under specific conditions. Understanding these pathways is essential for developing therapeutic strategies targeting smooth muscle disorders, such as hypertension or asthma, where dysregulation of cyclic nucleotide signaling often plays a significant role.
Meds and Muscle Problems: What's the Link?
You may want to see also
Explore related products






![]()
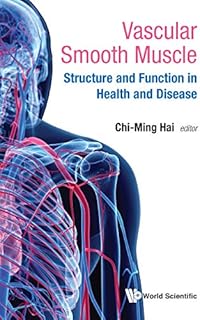
Calcium-Sensing Receptors (CaSR)
The signaling pathway triggered by CaSR activation involves the coupling of the receptor to G proteins, primarily Gq/11. Upon activation, Gq/11 stimulates phospholipase C (PLC), which hydrolyzes phosphatidylinositol 4,5-bisphosphate (PIP₂) into inositol trisphosphate (IP₃) and diacylglycerol (DAG). IP₃ binds to its receptors on the endoplasmic reticulum, causing the release of calcium ions into the cytoplasm. This increase in intracellular calcium activates calcium-calmodulin-dependent kinase II (CaMKII) and myosin light chain kinase (MLCK), leading to phosphorylation of the myosin light chain (MLC) and subsequent smooth muscle contraction. DAG, on the other hand, activates protein kinase C (PKC), which can further modulate the contractile machinery and enhance the contractile response.
In addition to its role in calcium-mediated contraction, CaSR signaling can also interact with other pathways to regulate smooth muscle tone. For example, CaSR activation can modulate the activity of voltage-gated calcium channels and transient receptor potential (TRP) channels, thereby influencing calcium influx and intracellular calcium dynamics. This cross-talk between CaSR and other signaling systems allows for fine-tuned regulation of smooth muscle contraction in response to changes in extracellular calcium levels. Such integration is particularly important in maintaining vascular tone and blood pressure, where CaSRs act as sensors of local calcium concentrations to adjust smooth muscle activity accordingly.
Pharmacological modulation of CaSRs presents a potential therapeutic avenue for conditions involving abnormal smooth muscle contraction, such as hypertension and asthma. Agonists and antagonists of CaSRs can be used to either enhance or inhibit smooth muscle contractility, depending on the clinical need. For instance, CaSR agonists could be employed to induce vasoconstriction in hypotensive states, while antagonists might be beneficial in reducing excessive smooth muscle contraction in hypertensive or hyperreactive airway disorders. Understanding the specific roles of CaSRs in different smooth muscle tissues is essential for developing targeted therapies that minimize off-target effects.
In summary, Calcium-Sensing Receptors (CaSR) represent a distinct signaling mechanism that contributes to smooth muscle contraction by responding to extracellular calcium levels. Through G protein-mediated pathways, CaSR activation increases intracellular calcium, leading to the phosphorylation of contractile proteins and muscle contraction. The receptor's ability to interact with other signaling systems enhances its regulatory role in smooth muscle function, making it a critical player in physiological processes such as vascular tone regulation. Further research into CaSRs and their modulation holds promise for advancing treatments for disorders characterized by dysregulated smooth muscle contractility.
Fosamax: Joint and Muscle Pain Side Effects?
You may want to see also
Explore related products






![]()
Mechanotransduction Mechanisms
Another important mechanotransduction mechanism is the activation of stretch-activated ion channels. These channels, such as transient receptor potential (TRP) channels, open in response to mechanical deformation of the cell membrane. The influx of cations, particularly calcium and sodium, depolarizes the cell membrane, triggering voltage-gated calcium channels to open further. This increase in intracellular calcium concentration activates calmodulin and myosin light chain kinase (MLCK), leading to phosphorylation of the myosin light chain and subsequent smooth muscle contraction. Stretch-activated channels thus provide a direct link between mechanical stimuli and the contractile machinery of the cell.
Cytoskeletal remodeling also plays a significant role in mechanotransduction-induced smooth muscle contraction. Mechanical forces applied to the cell can alter the organization of actin and intermediate filaments, which are connected to focal adhesions and integrins. These changes in cytoskeletal structure transmit signals to intracellular proteins such as Rho kinase (ROCK) and focal adhesion kinase (FAK). ROCK, in particular, activates MLCK and inhibits myosin phosphatase, enhancing myosin light chain phosphorylation and promoting contraction. This mechanism demonstrates how mechanical stress can modulate cytoskeletal dynamics to regulate contractility.
Additionally, extracellular matrix (ECM) interactions contribute to mechanotransduction in smooth muscle cells. Integrins, which are transmembrane proteins linking the ECM to the cytoskeleton, act as mechanosensors. When mechanical forces are applied, integrins cluster and recruit adaptor proteins, initiating signaling cascades that involve proteins like Src kinase and focal adhesion kinase. These signals can lead to the activation of small GTPases such as RhoA, which further enhances ROCK activity and promotes contraction. The ECM thus serves as both a structural scaffold and a signaling hub in response to mechanical stimuli.
Finally, caveolae—small invaginations in the plasma membrane enriched in caveolin proteins—are emerging as important mechanotransducers in smooth muscle cells. Caveolae act as mechanosensitive structures that flatten in response to stretch, leading to the release of caveolin and the activation of downstream signaling pathways. Caveolin can interact with proteins like endothelial nitric oxide synthase (eNOS) and G proteins, modulating calcium signaling and contractile responses. This mechanism underscores the complexity of how smooth muscle cells integrate mechanical cues to regulate contraction.
In summary, mechanotransduction mechanisms in smooth muscle contraction involve a diverse array of processes, including GPCR activation, stretch-activated ion channels, cytoskeletal remodeling, ECM interactions, and caveolae-mediated signaling. These pathways collectively ensure that mechanical stimuli are efficiently translated into biochemical signals, ultimately driving the contractile function of smooth muscle cells. Understanding these mechanisms provides valuable insights into both physiological and pathological conditions involving smooth muscle contractility.
Botox and Muscle Atrophy: What's the Real Deal?
You may want to see also
Frequently asked questions
Calcium signaling is a primary mechanism for smooth muscle contraction. An increase in intracellular calcium concentration activates calmodulin, which then binds to myosin light-chain kinase (MLCK). This leads to phosphorylation of myosin light chains, enabling actin-myosin interaction and muscle contraction.
Acetylcholine binds to muscarinic receptors on smooth muscle cells, activating the IP3/DAG pathway. This results in the release of calcium from the sarcoplasmic reticulum, increasing intracellular calcium levels and triggering contraction via the same calcium-dependent mechanisms.
Yes, Rho-kinase signaling is another important pathway. It phosphorylates the myosin light-chain phosphatase (MLCP), reducing its activity and leading to sustained phosphorylation of myosin light chains. This enhances actin-myosin interactions and promotes smooth muscle contraction independently of calcium.