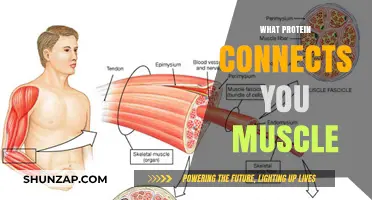
Muscle loss, or muscle atrophy, is a serious condition that can be caused by a variety of factors, including certain medications, ageing, and underlying health conditions. While there are prescription medications that can cause muscle loss, there are also treatments available to mitigate this. For example, cholesterol-lowering drugs such as statins and fibrates can cause drug-induced myopathy, which leads to muscle weakness, pain, inflammation, stiffness, spasms, and cramps. On the other hand, medications such as bimagrumab have been shown to increase muscle mass in older adults with sarcopenia, a syndrome characterized by the progressive loss of skeletal muscle mass and function. Additionally, lifestyle changes such as resistance training and increased protein intake can help prevent muscle loss while losing weight.
Explore related products






What You'll Learn
![]()
Drugs for treating muscle atrophy
Muscle atrophy, or the wasting and thinning of muscle mass, can be caused by muscle disuse or neurogenic conditions. While there is currently no drug approved to treat skeletal muscle atrophy, there are some treatments that can help prevent, attenuate, or reverse muscle atrophy.
Disuse atrophy can often be reversed with exercise and a healthy diet. A healthcare provider may recommend physical therapy or an exercise plan, which could include exercises in a pool to reduce muscle workload. Nutritional supplements may also be suggested.
Neurogenic atrophy is caused by an injury or disease affecting the nerves that connect to the muscles. When these nerves are damaged, they cannot trigger the muscle contractions needed to stimulate muscle activity, so the body starts breaking down the muscles, causing them to decrease in size and strength. This type of atrophy can sometimes be treated with a special kind of physical therapy called electrical stimulation.
Some studies have shown that administering anti-murine TNF IgG in rats can reduce circulating TNF-α and inhibit muscle protein degradation. Similarly, injecting soluble TNF receptors (sTNFR1, a specific inhibitor of TNF-α) can prevent the interaction of TNF-α with its receptor, thereby reducing skeletal muscle waste and preserving body weight.
In terms of drugs, a phase I trial of GSK2881078 for the treatment of weakness caused by COPD has been completed, and the development of SARM drugs is ongoing. Ghrelin, a growth hormone-releasing polypeptide, has been shown to reduce dexamethasone-, fasting-, denervation-, cancer-, and cisplatin-induced muscle atrophy.
Other potential treatments include enalapril, which can reduce the risk of weight loss and delay cachexia, and perindopril, which has been shown to improve physical function in the elderly. Intravenous MABp1 treatment has been shown to increase lean body mass and improve quality of life in adults with metastatic solid cancer, although there was no control group in this study.
Vegan Muscle Power: Fact or Fiction?
You may want to see also
Explore related products





![]()
Medication causing muscle weakness
Muscle weakness can be caused by a variety of factors, including chronic conditions, infections, and medication. While medication-induced muscle weakness may be rare, it is a possibility that should not be overlooked.
Medications that are known to cause muscle weakness include statins, which are a class of drugs used to lower cholesterol. Simvastatin and atorvastatin are examples of statins that can lead to muscle weakness and even rhabdomyolysis, a severe condition where muscle fibers break down and can cause kidney damage. Beta-blockers, which are commonly prescribed for cardiovascular issues, can also cause muscle weakness and cramps. Additionally, antiarrhythmic medications like amiodarone and procainamide, used to treat heart rhythm problems, have been linked to muscle weakness. Corticosteroids, such as prednisone, especially when taken in high doses or for extended periods, may also induce muscle weakness.
Other medications that have been associated with muscle weakness include anti-retroviral drugs like zidovudine, which can lead to mitochondrial myopathies affecting the genetic material in muscle cells. Diuretics or water pills can cause muscle weakness by inducing hypokalemia or low potassium levels. While it is uncommon, blood pressure medications, including beta-blockers, have been known to cause fatigue and weakness in some cases. Furthermore, D-penicillamine, an anti-inflammatory drug, has also been linked to drug-induced myopathy.
It is important to note that not all individuals taking these medications will develop muscle weakness, and the occurrence of this side effect varies. However, if you experience muscle weakness while taking any medication, it is crucial to consult your doctor. They can evaluate your symptoms, adjust your medication dosage, or recommend alternative treatments.
Muscle Beach: A Cultural Icon of Fitness
You may want to see also
Explore related products






![]()
Oral drugs causing muscle wasting
Sarcopenia is a geriatric syndrome characterised by progressive and generalised loss of skeletal muscle mass and function. The reported prevalence of this syndrome differs depending on the definition, the population, and the method used to identify sarcopenia. The causes of sarcopenia are multifactorial and can include genetic influence, immobility, endocrine factors, inflammation, and nutritional deficiencies. These disorders involve an imbalance between anabolic and catabolic pathways that govern muscle mass. Many drugs taken regularly for common conditions may interact with some mechanisms that can alter the balance between protein synthesis and degradation, leading to a harmful or beneficial effect on muscle mass and strength.
Widely prescribed drugs could play an important role in the onset and development of sarcopenia. For example, anti-diabetic agents have been associated with sarcopenia and osteosarcopenia in Iranian older adults. Statins, which are cholesterol-lowering drugs, have been linked to muscle weakness and necrotizing myopathy, characterised by the death of muscle fibres. Fibrates, such as fenofibrate and gemfibrozil, are another class of cholesterol-lowering drugs that have been associated with muscle weakness. Antiarrhythmic medicines used to treat heart rhythm problems, such as amiodarone and procainamide, have also been implicated in causing muscle weakness. Corticosteroids, particularly when taken in high doses or for prolonged periods, can lead to muscle weakness and pain.
In addition to the above, other oral drugs have been associated with muscle wasting and sarcopenia. Glucocorticoid therapy and intensive care treatments have been linked to skeletal muscle wasting, although the specific mechanisms are not yet fully understood. Antiepileptic drugs such as lamotrigine and phenytoin, as well as omeprazole, a medication for gastroesophageal reflux disease (GERD), have been linked to a small number of cases of drug-induced myopathy. It is important to note that not all individuals taking these medications will develop muscle problems, and the benefits and risks should be discussed with a doctor.
While there is no approved drug therapy for sarcopenia-related muscle wasting, some studies have shown that targeting Dual Specificity Phosphatase 22 (DUSP22) through knockdown or pharmacological inhibition can prevent multiple forms of muscle wasting.
Sleep: Muscle Repair and Recovery
You may want to see also
Explore related products





![]()
Treatments for muscle atrophy in COPD
Muscle atrophy is a common complication of chronic obstructive pulmonary disease (COPD), a progressive lung disease that affects a significant number of people globally. COPD patients experience skeletal muscle dysfunction, often accompanied by muscle mass loss, which severely impacts their quality of life and survival. The complexity of muscle wasting in COPD involves multiple factors, including inflammatory cytokines, oxidative stress, hormonal imbalances, nutritional deficiencies, and reduced physical activity. While there is currently no cure for COPD-related lung pathology, emerging treatments offer hope for tackling muscle atrophy and improving patients' overall well-being.
Disuse, hypoxemia, malnutrition, oxidative stress, and systemic inflammation are among the key contributors to muscle atrophy in COPD. Systemic inflammation, in particular, plays a significant role in disease progression, and anti-inflammatory drugs, such as corticosteroids, are often prescribed to counter this aspect. However, prolonged corticosteroid use can lead to "steroid myopathy," characterized by type II fiber atrophy. As such, alternative treatments are being explored, including the vitamin D analogue α-calcidol, which has shown promise in reducing circulating TNF-α levels and improving muscle power in patients with rheumatoid arthritis.
Pharmacological therapies under development for muscle atrophy in other pathological states may also hold relevance for treating muscle wasting in COPD patients. For instance, the ubiquitin-proteasome system, which plays a role in muscle atrophy, can be blocked by proteasome inhibitors, although their effectiveness in preserving muscle mass under catabolic conditions requires further study. Additionally, the IGF-1/PI3K/Akt/mTOR pathway, associated with anabolic processes, can be targeted for muscle hypertrophy, but it is not currently used as a drug target.
Beyond pharmacological interventions, addressing nutritional abnormalities and physical inactivity is crucial for managing muscle atrophy in COPD patients. Nutritional deficiencies, including malnutrition, can exacerbate muscle wasting, emphasizing the importance of adequate dietary intake. Furthermore, physical inactivity or disuse can contribute to muscle atrophy, making it essential to encourage and assist patients in maintaining an appropriate level of physical activity to help preserve muscle mass and function.
In summary, treatments for muscle atrophy in COPD patients encompass both pharmacological and non-pharmacological approaches. While anti-inflammatory medications like corticosteroids are commonly used, their long-term effects may be detrimental, highlighting the need for alternative drug therapies. Exploring the potential of existing treatments for other conditions, such as α-calcidol, could provide new avenues for managing muscle atrophy in COPD. Additionally, addressing nutritional deficiencies and promoting physical activity are vital components of a comprehensive treatment strategy to improve the quality of life for individuals living with COPD.
Understanding Your Core Muscles: Definition and Benefits
You may want to see also
Explore related products






![]()
Preventing muscle loss during weight loss
Losing weight can mean losing both fat and muscle. However, there are ways to prevent muscle loss during weight loss.
Firstly, it is important to focus on improving muscle quality rather than preserving or increasing muscle mass. This can be achieved through resistance training, which is one of the most important factors in maintaining muscle mass during weight loss. Resistance training two to three times a week for up to six months has been shown to prevent muscle loss while reducing fat mass and body weight. Additionally, aerobic exercises can be incorporated with resistance training to benefit fat loss and preserve muscle mass. However, it is important to limit the amount of cardio performed before resistance training.
Secondly, protein intake plays a crucial role in preventing muscle loss. Experts recommend spreading protein intake evenly throughout the day and aiming for 1.2 to 1.6 grams of protein per kilogram of body weight. For those who exercise frequently, older individuals, or those on a weight loss journey, protein intake may need to be increased to more than 2 grams per kilogram of body weight. However, it is important not to exceed 2.5 grams per kilogram of body weight, as excessive protein intake can have adverse effects on metabolism and may lead to liver and kidney damage.
Finally, consuming certain supplements may help improve muscle mass, recovery, and strength while promoting fat loss. Caffeine and nitrate supplements taken before exercising can boost muscular strength and help preserve muscle mass. However, it is important to consult with a healthcare professional before taking any supplements, as they may negatively interact with certain medications or conditions.
In conclusion, by combining resistance training with adequate protein intake and careful supplementation, individuals can effectively prevent muscle loss during weight loss.
Muscle Glycogen: The Energy Source for Muscles Explained
You may want to see also
Frequently asked questions
Prescription drugs that can cause muscle loss include cholesterol-lowering drugs such as statins and fibrates, and antiarrhythmic medicines. Other drugs that can cause muscle loss include Ozempic and Wegovy, which are weight loss medications.
Bimagrumab is a drug that has been shown to increase muscle mass in older adults with sarcopenia. MABp1 is another drug that has been shown to increase lean body mass in patients with advanced colorectal cancer. Other drugs that can help treat muscle loss include enalapril and perindopril.
Increasing protein intake and incorporating strength and resistance training can help prevent muscle loss. It is recommended to consume 25-30 grams of protein per meal and include lean protein sources such as chicken breast and low/non-fat Greek yogurt.