The rotator cuff is a group of four muscles that play a crucial role in stabilizing and moving the shoulder joint. When discussing arm abduction, the specific rotator cuff muscle responsible for this movement is the supraspinatus. The supraspinatus initiates the abduction of the arm by lifting it away from the body, particularly in the first 15 degrees of the motion. While other muscles, such as the deltoid, contribute to the full range of abduction, the supraspinatus is essential for starting the movement and maintaining proper shoulder mechanics. Understanding its function is vital for assessing shoulder health and addressing injuries related to arm abduction.
| Characteristics | Values |
|---|---|
| Muscle Name | Supraspinatus |
| Action | Primary abductor of the arm (initiates abduction from 0° to 15°) |
| Origin | Supraspinous fossa of the scapula |
| Insertion | Greater tubercle of the humerus (via supraspinatus tendon) |
| Nerve Supply | Suprascapular nerve (C5, C6) |
| Function | Initiates arm abduction, stabilizes glenohumeral joint |
| Common Injuries | Rotator cuff tears, impingement syndrome |
| Synergists | Deltoid (middle fibers), other rotator cuff muscles (during abduction) |
| Antagonists | Latissimus dorsi, teres major, pectoralis major (during adduction) |
Explore related products





What You'll Learn
![]()
Supraspinatus role in abduction
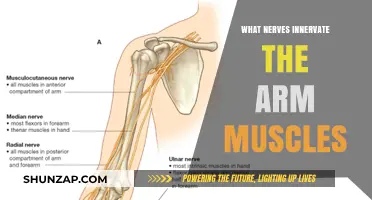
The supraspinatus muscle, one of the four rotator cuff muscles, plays a critical role in arm abduction, particularly in the initial phase of lifting the arm away from the body. Located on the upper back, it originates in the supraspinous fossa of the scapula and inserts on the greater tubercle of the humerus. Its primary function is to initiate abduction of the arm, contributing to the first 15 degrees of this movement. Beyond this range, the deltoid muscle takes over as the primary abductor, but the supraspinatus remains essential for stabilizing the humeral head within the glenoid fossa during the entire range of motion.
From an anatomical perspective, the supraspinatus is uniquely positioned to perform its role. Its tendon passes beneath the acromion, a bony projection on the scapula, making it susceptible to impingement, especially during repetitive overhead activities. This vulnerability highlights the importance of maintaining proper shoulder mechanics to avoid injury. For instance, athletes in sports like swimming, tennis, or baseball, where overhead motions are frequent, should incorporate strengthening exercises for the supraspinatus to prevent strains or tears. A practical tip is to perform external rotation exercises with a resistance band, ensuring the elbow is tucked into the side to isolate the rotator cuff muscles effectively.
Instructively, rehabilitating a supraspinatus injury often involves a phased approach. Initially, focus on reducing pain and inflammation through rest, ice, and anti-inflammatory medications. Once acute symptoms subside, gentle range-of-motion exercises, such as pendulum swings, can help restore mobility. The next phase emphasizes strengthening, starting with isometric exercises like wall presses, progressing to resisted external rotation with light weights or bands. Advanced stages may include functional movements that mimic daily or sport-specific activities. Caution should be taken to avoid overloading the muscle, as premature return to high-intensity activities can lead to re-injury.
Comparatively, while the supraspinatus is vital for abduction, it works in tandem with the other rotator cuff muscles—infraspinatus, teres minor, and subscapularis—to provide dynamic stability to the shoulder joint. Unlike the supraspinatus, which primarily assists in abduction, the infraspinatus and teres minor are external rotators, while the subscapularis is an internal rotator. This coordinated effort ensures the humeral head remains centered during movement, preventing dislocation or wear on the joint surfaces. Understanding this interplay is crucial for designing comprehensive shoulder strengthening programs, especially for individuals recovering from injury or seeking to enhance athletic performance.
Descriptively, the supraspinatus tendon’s role in abduction can be likened to a pulley system, where it acts as the initial lever to lift the arm. Imagine lifting a heavy curtain—the first tug requires the most effort, similar to the supraspinatus initiating abduction. As the arm rises, the deltoid takes over, much like the curtain’s weight shifting to a secondary mechanism. This analogy underscores the supraspinatus’s indispensable yet often underappreciated function. For those experiencing shoulder pain during abduction, a simple self-test involves attempting to lift the arm while someone applies gentle downward pressure—weakness or pain may indicate supraspinatus involvement, warranting further evaluation by a healthcare professional.
Effective Healing Tips for a Sprained Arm Muscle Recovery
You may want to see also
Explore related products




![]()
Shoulder abduction mechanics
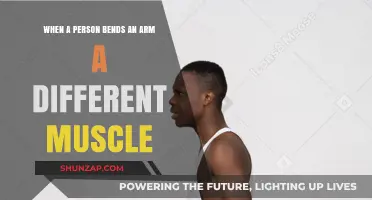
The supraspinatus muscle, a key player in the rotator cuff, is primarily responsible for initiating arm abduction. This action begins the movement of lifting your arm away from your body, but it’s not a solo effort. As the arm rises above 15 degrees, the deltoid muscle takes over as the primary mover, while the supraspinatus assists by stabilizing the humeral head in the glenoid fossa. This mechanical interplay highlights the importance of both strength and coordination in shoulder function. Without proper supraspinatus engagement, even simple tasks like reaching for a shelf or lifting a bag can become inefficient or painful.
Analyzing the mechanics further, shoulder abduction occurs in the scapular plane, an angle approximately 30 degrees forward of the sagittal plane. This position minimizes stress on the joint while maximizing force production. For optimal performance, exercises like cable lateral raises or resistance band abduction should mimic this plane. A common mistake is allowing the arm to drift forward, which overloads the anterior shoulder structures and reduces the effectiveness of the movement. Incorporating a slight external rotation of the arm during abduction can enhance supraspinatus activation, a technique particularly useful for athletes or those in rehabilitation.
From a practical standpoint, strengthening the supraspinatus and its rotator cuff companions is crucial for injury prevention. For adults aged 30–60, incorporating 2–3 sets of 12–15 repetitions of isolated abduction exercises twice weekly can maintain shoulder health. Lightweight (2–5 lbs) is recommended to avoid strain, especially for beginners. Advanced individuals can progress to isometric holds or eccentric training, which have been shown to improve muscle endurance and joint stability. Caution should be taken to avoid overtraining, as the supraspinatus is prone to tendinopathy from repetitive stress.
Comparatively, while the supraspinatus dominates the initial phase of abduction, the infraspinatus and teres minor contribute by providing external rotation, which subtly assists in the movement. This highlights the rotator cuff’s role as a synergistic unit rather than isolated muscles. For instance, a study in the *Journal of Shoulder and Elbow Surgery* found that athletes with balanced rotator cuff strength had a 40% lower risk of shoulder injuries. This underscores the need for comprehensive training programs that address all cuff muscles, not just the primary abductors.
Descriptively, imagine the shoulder as a ball-and-socket joint where the humeral head (ball) must remain centered during abduction. The supraspinatus acts like a tether, pulling the head upward and outward while the other cuff muscles stabilize it. This dynamic process is akin to balancing a marble on a spoon—precision is key. Visualizing this mechanism can help individuals perform exercises with greater mindfulness, ensuring each movement reinforces proper alignment. For those recovering from injury, focusing on this imagery can accelerate recovery by promoting neuromuscular re-education.
Effective Techniques to Loosen Arm Muscles During Climbing Adventures
You may want to see also
Explore related products





![]()
Supraspinatus vs. other muscles
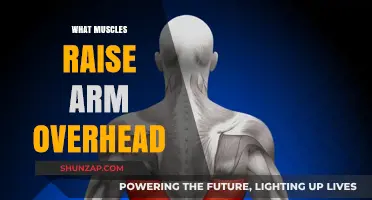
The supraspinatus muscle is often the first to come to mind when discussing arm abduction within the rotator cuff group, but its role is more nuanced than commonly assumed. While it initiates abduction by moving the arm away from the body, its primary function is to stabilize the humeral head within the glenoid fossa, preventing impingement during movement. This stabilization is crucial for smooth, pain-free motion, especially in the initial 0-15 degrees of abduction. Beyond this range, other muscles, such as the deltoid, take over as the primary movers, highlighting the supraspinatus’s specialized role.
In contrast to the supraspinatus, the deltoid muscle is the powerhouse of arm abduction, responsible for the majority of the movement from 15 to 180 degrees. Unlike the supraspinatus, which originates on the scapula and inserts on the humerus, the deltoid’s broader origin and insertion allow it to generate significant force. However, this strength comes at a cost: the deltoid’s bulk can sometimes overshadow the supraspinatus, leading to overuse injuries if the latter is weak or compromised. For instance, athletes or individuals performing repetitive overhead motions should focus on supraspinatus-specific exercises, like external rotation with a resistance band, to maintain balance and prevent impingement syndromes.
Another rotator cuff muscle, the infraspinatus, often gets grouped with the supraspinatus due to their proximity and shared role in shoulder stability. However, the infraspinatus primarily externally rotates the arm, a function distinct from abduction. While both muscles work together to stabilize the shoulder joint, the supraspinatus’s unique position above the spine of the scapula makes it more susceptible to injury, particularly in activities involving lifting or throwing. Strengthening both muscles is essential, but exercises like prone external rotation with a dumbbell target the infraspinatus more effectively, ensuring it doesn’t compensate for a weak supraspinatus.
The subscapularis, the largest and strongest rotator cuff muscle, internally rotates the arm and stabilizes the joint from the front. Unlike the supraspinatus, which is more vulnerable due to its smaller size and tendon’s passage through the subacromial space, the subscapularis’s robust structure makes it less prone to injury. However, its role in abduction is minimal, emphasizing the supraspinatus’s irreplaceable function in the initial phase of movement. For individuals recovering from rotator cuff injuries, focusing on supraspinatus rehabilitation, such as isometric holds or light cable rows, is critical before progressing to more complex exercises involving the subscapularis.
In practical terms, understanding the distinct roles of these muscles allows for targeted training and injury prevention. For example, a physical therapist might prescribe supraspinatus-specific exercises like empty cans or full cans to isolate and strengthen this muscle, while cautioning against overloading the deltoid in early recovery phases. By appreciating the supraspinatus’s unique contribution to abduction and stability, individuals can maintain shoulder health and optimize performance in both daily activities and sports. This nuanced approach ensures that the supraspinatus isn’t overshadowed by its larger counterparts, preserving the delicate balance of the rotator cuff system.
Is the Arm's Cardiac Muscle a Myth or Reality?
You may want to see also
Explore related products






![]()
Abduction range of motion
The supraspinatus muscle, one of the four rotator cuff muscles, is primarily responsible for initiating arm abduction. However, achieving a full abduction range of motion (ROM) requires coordinated effort from multiple muscles, including the deltoid, trapezius, and serratus anterior. Understanding this interplay is crucial for optimizing shoulder function and preventing injury.
Abduction ROM is typically measured from the anatomical position (arm at the side) to full overhead elevation, totaling approximately 180 degrees. This range can be divided into three phases: initial abduction (0-30 degrees), mid-range abduction (30-90 degrees), and full abduction (90-180 degrees). Each phase relies on different muscular contributions, with the supraspinatus dominant in the initial phase and the deltoid becoming increasingly involved as the arm elevates.
Age, injury, and lifestyle factors significantly impact abduction ROM. Studies show a natural decline in shoulder flexibility with age, with individuals over 60 experiencing an average 20-degree reduction in abduction compared to younger adults. Athletes and individuals with physically demanding jobs often exhibit greater ROM due to consistent use and training. Conversely, sedentary lifestyles and conditions like adhesive capsulitis (frozen shoulder) can lead to significant ROM restrictions.
To maintain or improve abduction ROM, incorporate specific exercises into your routine. Start with isometric holds at various abduction angles, progressing to resistance band exercises like lateral raises and external rotations. Aim for 3 sets of 10-15 repetitions, 2-3 times per week. For individuals with limited ROM, gentle stretching exercises like the sleeper stretch or cross-body stretch can help improve flexibility. Always prioritize proper form and avoid forcing movements beyond your current capacity to prevent strain.
Regularly assessing your abduction ROM using a goniometer or visual estimation can help track progress and identify potential issues early on. If you experience persistent pain or significant ROM limitations, consult a healthcare professional for a thorough evaluation and personalized treatment plan. Remember, maintaining optimal shoulder mobility is essential for performing daily activities and preventing injuries.
Understanding the Biceps Brachii: Anterior Upper Arm Muscle Explained
You may want to see also
Explore related products






![]()
Supraspinatus injury impact
The supraspinatus muscle, a key player in the rotator cuff, is primarily responsible for initiating arm abduction, lifting the arm away from the body. When injured, this muscle's function is compromised, leading to significant impairments in shoulder mobility and strength. A supraspinatus injury often results from repetitive overhead activities, acute trauma, or degenerative changes, particularly in individuals over 40. Understanding the impact of such an injury is crucial for effective management and recovery.
Analyzing the Impact:
A supraspinatus injury typically manifests as pain during arm abduction, especially in the initial 15 to 60 degrees of movement, known as the "painful arc." This limitation disrupts daily activities like reaching for objects, combing hair, or lifting items overhead. Weakness in the injured shoulder becomes evident, often accompanied by a sensation of instability or "giving way." Over time, disuse of the arm can lead to muscle atrophy and further functional decline. For athletes or workers reliant on overhead movements, this injury can sideline them for weeks or even months, depending on severity.
Practical Management Steps:
Initial treatment focuses on reducing pain and inflammation, often involving rest, ice, and anti-inflammatory medications like ibuprofen (200–400 mg every 6–8 hours, as needed). Physical therapy is critical, emphasizing gentle range-of-motion exercises to maintain flexibility and progressive strengthening to restore supraspinatus function. For example, external rotation exercises with a resistance band (2–3 sets of 10–15 repetitions daily) can help rebuild strength. Corticosteroid injections may be considered for persistent pain, but their overuse should be avoided due to potential tendon weakening.
Comparative Considerations:
Unlike injuries to other rotator cuff muscles, supraspinatus tears are more likely to cause isolated abduction deficits, whereas subscapularis or infraspinatus injuries affect internal or external rotation, respectively. This specificity makes diagnosis and targeted rehabilitation more straightforward. However, chronic supraspinatus injuries may progress to larger tears, increasing the likelihood of surgical intervention. Arthroscopic repair, with a success rate of 85–90%, is often recommended for full-thickness tears, especially in active individuals under 60.
Preventive Measures and Takeaway:
To minimize the risk of supraspinatus injury, incorporate shoulder-strengthening exercises into your routine, focusing on the rotator cuff and scapular stabilizers. Avoid repetitive overhead activities without adequate rest, and ensure proper technique during sports or work tasks. For those over 40, regular stretching and gradual progression in activity intensity can help prevent degenerative changes. Early intervention is key—ignoring persistent shoulder pain can lead to irreversible damage. By understanding the unique impact of a supraspinatus injury, individuals can take proactive steps to preserve shoulder health and function.
Sculpt & Define: Enhancing Arm Muscles with Makeup Techniques
You may want to see also
Frequently asked questions
The supraspinatus muscle is the primary rotator cuff muscle responsible for initiating arm abduction.
The supraspinatus assists in lifting the arm away from the body (abduction) by stabilizing the shoulder joint and helping the deltoid muscle perform this movement.
Yes, the deltoid muscle is the main abductor of the arm, but the supraspinatus plays a crucial supporting role in the initial phase of abduction.
An injured supraspinatus can lead to weakness, pain, and difficulty in lifting the arm, particularly in the first 15 degrees of abduction.