The glenohumeral joint, also known as the shoulder joint, is a ball-and-socket joint that connects the upper limb to the axial skeleton or trunk. It is formed by the articulation of the scapula and the humerus, with the humeral head lying within the glenoid fossa of the scapula. This joint is one of the most mobile in the human body, allowing for a wide range of motion across multiple planes, including flexion, extension, abduction, adduction, and internal/external rotation. However, this mobility comes at the cost of stability, and the glenohumeral joint is susceptible to injuries and dislocations. The joint is surrounded by several muscles, including the rotator cuff muscles, deltoid muscles, and biceps brachii, which play a crucial role in stabilising the joint and facilitating its movements.
| Characteristics | Values |
|---|---|
| Joint Type | Ball and socket synovial joint |
| Bones | Scapula and Humerus |
| Ligaments | Coracohumeral, Glenohumeral, Transverse Humeral, Superior, Middle, and Inferior Glenohumeral |
| Nerves | Suprascapular, Lateral Pectoral, and Axillary |
| Muscles | Rotator Cuff (Supraspinatus, Infraspinatus, Subscapularis, and Teres Minor), Deltoid, Biceps Brachii, Latissimus Dorsi, Pectoralis Major, Triceps Brachii, and Scapulothoracic Musculature |
| Planes of Movement | Axial, Sagittal, Coronal, and Scapular |
| Range of Motion | Flexion (180°), Extension (45°-60°), Internal Rotation (70°-90°), Abduction, Adduction, External/Lateral Rotation, Circumduction |
| Stability | Least stable joint in the body |
Explore related products






What You'll Learn
![]()
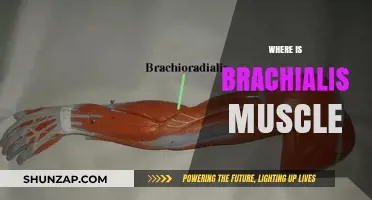
Glenohumeral joint anatomy
The glenohumeral joint, also known as the shoulder joint, is a ball-and-socket joint that connects the upper limb to the axial skeleton. It is formed by the articulation of the head of the humerus and the glenoid cavity (or fossa) of the scapula. The glenoid cavity is shallow and oval-shaped, and it is reinforced by a fibrocartilaginous rim called the glenoid labrum, which deepens its concavity to enhance joint stability. The head of the humerus is much larger than the glenoid fossa, allowing for a wide range of motion, including flexion, extension, abduction, adduction, external/lateral rotation, internal/medial rotation, and circumduction.
The glenohumeral joint is a synovial joint, meaning that the articulating surfaces are covered with hyaline cartilage. The synovial membrane lines the inner surface of the joint capsule and produces synovial fluid, which reduces friction between the articular surfaces. The joint capsule is lax, allowing for greater mobility, especially in abduction movements. However, this mobility comes at the cost of stability, and the surrounding muscles, ligaments, and ligamentous structures provide essential reinforcement and security to the joint.
Several ligaments play a crucial role in stabilising the glenohumeral joint and resisting humeral dislocation. These include the coracohumeral ligament, which extends from the coracoid process of the scapula to the tubercles of the humerus, and the transverse humeral ligament, which extends between the two tubercles of the humerus. The glenohumeral ligaments (superior, middle, and inferior) extend from the humerus to the glenoid fossa, reinforcing the joint capsule and stabilising the anterior aspect of the joint.
The rotator cuff muscles, including the supraspinatus, infraspinatus, teres minor, and subscapularis, also contribute to the stability of the glenohumeral joint. They form a sleeve around the anterior, superior, and posterior humeral head and glenoid cavity, compressing the joint and providing additional mobility. The tendons of these muscles blend with the joint capsule, forming a continuous structure that further stabilises the joint.
Lungs: Muscular or Not?
You may want to see also
Explore related products






![]()
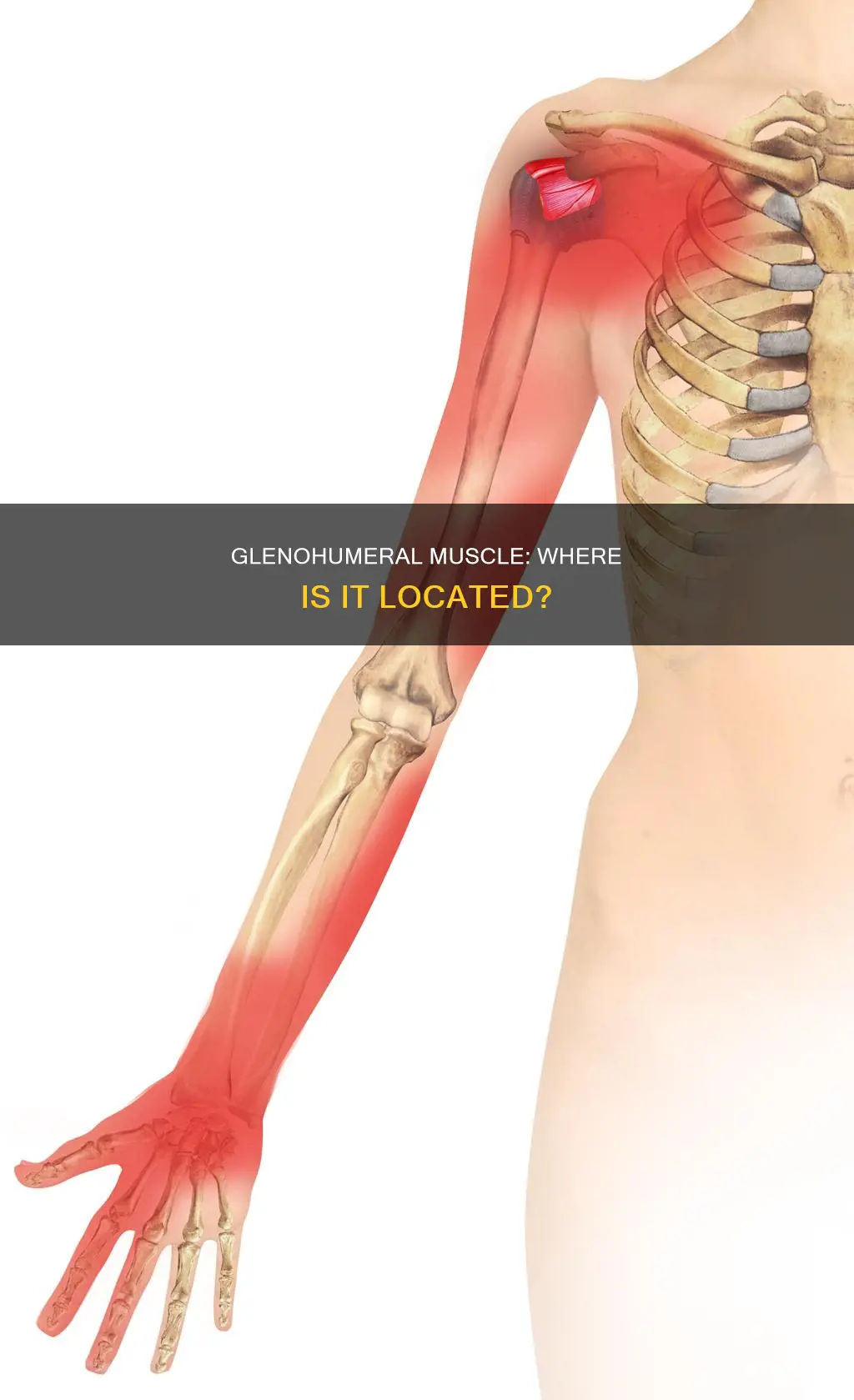
Glenohumeral joint mobility
The glenohumeral joint, or shoulder joint, is a ball-and-socket joint that attaches the upper limb to the axial skeleton. It is formed between the glenoid fossa of the scapula and the head of the humerus. The shoulder joint is the most mobile joint in the human body, allowing for a wide range of movements including flexion, extension, abduction, adduction, external/lateral rotation, internal/medial rotation, and circumduction. This range of motion comes at the cost of stability, as the bony surfaces of the joint offer little support. Instead, the joint relies on the surrounding muscles, ligaments, and tendons for stability.
The rotator cuff muscles play a crucial role in stabilising the glenohumeral joint. These muscles are often under heavy strain, making injuries relatively common. Rotator cuff pathologies include tendinitis, shoulder impingement, and sub-acromial bursitis. Tendinitis refers to inflammation of the muscle tendons, usually due to overuse, which can cause degenerative changes in the subacromial bursa and the supraspinatus tendon. This can lead to bursitis and impingement, characterised by pain in the middle of abduction between 60-120 degrees.
Several ligaments also contribute to the stability of the glenohumeral joint. The glenohumeral ligaments (superior, middle, and inferior) extend from the humerus to the glenoid fossa, reinforcing the joint capsule. The coracohumeral ligament extends from the base of the coracoid process to the greater tubercle of the humerus, supporting the superior part of the joint capsule. The transverse humeral ligament extends between the two tubercles of the humerus and holds the tendon of the long head of the biceps in the intertubercular groove.
Synovial fluid-filled bursae also assist with the joint's mobility. The subdeltoid-subacromial (SASD) bursa is located between the joint capsule and the deltoid muscle, while the subcoracoid bursae are found between the capsule and the coracoid process of the scapula. These bursae allow the structures of the shoulder joint to slide easily over one another, facilitating the joint's mobility.
The glenohumeral joint's extreme mobility comes with a trade-off in stability, making it one of the most frequently injured joints in the body. Understanding the joint's anatomy and the contributions of various muscles and ligaments to its movements is essential for differentiating shoulder pathologies and promoting joint health.
The Retina: A Muscle or Not?
You may want to see also
Explore related products






![]()
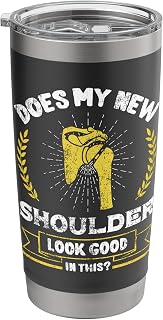
Glenohumeral joint stability
The glenohumeral joint, also known as the shoulder joint, is a ball-and-socket joint formed between the glenoid fossa of the scapula and the head of the humerus. It is one of the four joints that comprise the shoulder complex and is responsible for connecting the upper limb to the trunk. This joint is considered to be the most mobile and least stable joint in the body, offering a wide range of motion at the cost of stability.
The stability of the glenohumeral joint is a multifactorial process influenced by various anatomical and biomechanical factors. The relationship between the size of the humeral head and the scapular glenoid fossa allows for a wide range of motion but requires effective stabilizers to prevent dislocation. The glenoid fossa is deepened by a fibrocartilage rim called the glenoid labrum, which helps to reduce the disproportion in surfaces.
Several ligaments and tendons play a crucial role in maintaining glenohumeral joint stability. The joint capsule is reinforced by the superior, middle, and inferior glenohumeral ligaments, which form a Z-shaped pattern. These ligaments act as the main stabilizers of the shoulder joint, preventing dislocation of the humeral head. Additionally, the rotator cuff muscles, including the supraspinatus, infraspinatus, subscapularis, and teres minor, are essential for stabilizing the joint and are often under heavy strain, making injuries relatively common.
Other ligaments contributing to glenohumeral joint stability include the coracohumeral ligament, which resists superior displacement of the humeral head, and the transverse humeral ligament, which prevents displacement of the tendon from the intertubercular sulcus. The synovial membrane lines the inner surface of the joint capsule and produces synovial fluid, reducing friction between the articular surfaces.
Overall, the stability of the glenohumeral joint depends on the interaction of multiple factors, including bone anatomy, soft tissues, and the neuromuscular balance of the surrounding muscles.
Building Muscle Tone: Foods to Fuel Your Fitness
You may want to see also
Explore related products

$21.99


$21.99

$21.99


![]()
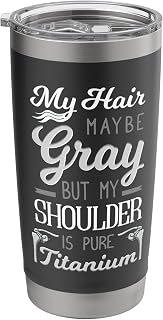
Glenohumeral joint injuries
The glenohumeral joint, also known as the shoulder joint, is a ball-and-socket joint formed between the glenoid fossa of the scapula and the head of the humerus. It is the major joint connecting the upper limb to the trunk and is one of the most mobile joints in the human body. This mobility, however, comes at the cost of stability, making the glenohumeral joint one of the most frequently injured joints.
One of the most important components of the glenohumeral joint is the rotator cuff. The rotator cuff is a group of four muscles (supraspinatus, infraspinatus, subscapularis, and teres minor) that stabilise the joint by compressing the humeral head against the glenoid. These muscles are often under heavy strain, making injuries relatively common. Rotator cuff injuries can occur from direct trauma, falls, or wear and tear over time. Symptoms include tenderness, soreness, and pain when moving the shoulder, and in severe cases, the inability to raise the arm. Treatment for rotator cuff injuries may include rest, ice, compression, elevation (RICE), physical therapy, and nonsteroidal anti-inflammatory drugs (NSAIDs).
Another common injury associated with the glenohumeral joint is shoulder impingement. Impingement occurs when the shoulder muscles rub excessively against the acromion and coracoid, which are parts of the shoulder blade. Activities requiring excessive overhead arm motion can lead to impingement. If left untreated, impingement can cause tendinitis, a form of inflammation, and potentially lead to tears that may require surgery.
In addition to rotator cuff injuries and impingement, glenohumeral joint instability is also prevalent. This instability can result in dislocations, where the ball of the joint slips out of the socket. Recurrent instability can be treated with surgery to repair torn ligaments. Frozen shoulder is another condition that can develop following a period of shoulder immobility or due to underlying health conditions. It is characterised by extreme stiffness and pain in the shoulder, and treatment options include NSAIDs, cortisone shots, and physical therapy.
The Role of Actin in Cardiac Muscle Function
You may want to see also
Explore related products
$21.99

$21.99

$21.99

$21.99
![]()
Glenohumeral joint nerves
The glenohumeral joint, or shoulder joint, is a highly mobile ball-and-socket joint formed between the glenoid fossa of the scapula and the head of the humerus. It is the major joint connecting the upper limb to the trunk and axial skeleton. This joint has the greatest range of motion of all the body's joints, allowing for flexion, extension, abduction, adduction, external/lateral rotation, internal/medial rotation, and circumduction.
However, this wide range of motion comes at the cost of stability, as the bony surfaces offer little support. As a result, the glenohumeral joint is one of the most frequently injured joints in the body and is particularly susceptible to dislocation.
The nerves that supply the glenohumeral joint include the suprascapular, lateral pectoral, and axillary nerves. These nerves originate from the brachial plexus, a nerve network formed by the ventral rami of C5 to T1. The axillary nerve is particularly vulnerable to injury during anterior dislocations of the glenohumeral joint, which can cause paralysis of the deltoid muscle and decreased sensation in the shoulder.
The suprascapular nerve innervates the supraspinatus and infraspinatus muscles, which primarily abduct the shoulder and contribute to external rotation, respectively. The axillary nerve supplies the teres minor muscle, which also contributes to external rotation. The subscapular nerve innervates the subscapularis muscle, which facilitates internal rotation.
The rotator cuff muscles play a crucial role in stabilising the glenohumeral joint. These muscles are often under heavy strain and are therefore susceptible to injuries such as tendinitis, impingement, and sub-acromial bursitis.
Massaging Your Triceps: Techniques for Relaxing This Muscle Group
You may want to see also
Frequently asked questions
The glenohumeral muscle is not a muscle but a joint. The glenohumeral joint is located in the shoulder.
The glenohumeral joint is a ball-and-socket joint that connects the upper limb to the trunk. It is formed between the glenoid fossa of the scapula and the head of the humerus.
The glenohumeral joint permits a wide range of motion across multiple planes. It is the most mobile joint in the human body but has little stability.
The rotator cuff muscles surround the glenohumeral joint and play a central role in stabilising it. The cuff is made up of the supraspinatus, infraspinatus, subscapularis, and teres minor muscles.