The suboccipital muscle group, located at the base of the skull, plays a crucial role in head and neck movements, particularly in extension and rotation. This group consists of four primary muscles: the rectus capitis posterior major, rectus capitis posterior minor, obliquus capitis superior, and obliquus capitis inferior. When discussing which muscle is not part of this group, it is important to consider the anatomical definitions and functions of these muscles. For instance, the trapezius muscle, while involved in head and neck movements, is not classified as part of the suboccipital group, as it primarily spans the upper back, neck, and shoulders, serving a broader range of functions beyond the specific actions of the suboccipital muscles. Understanding this distinction helps clarify the unique role of the suboccipital group in cervical mechanics.
Explore related products






What You'll Learn
- Rectus capitis posterior major: Not part of suboccipital group, but near it, attaching to spine
- Rectus capitis posterior minor: Also not in the group, assists neck extension and rotation
- Obliquus capitis superior: Included in suboccipital group, extends and rotates head
- Obliquus capitis inferior: Part of the group, aids in head tilting and rotation
- Semispinalis capitis: Not in suboccipital group, helps extend the head and neck
![]()
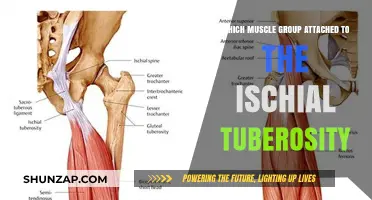
Rectus capitis posterior major: Not part of suboccipital group, but near it, attaching to spine
The Rectus capitis posterior major (RCPM) is often mistaken for a member of the suboccipital muscle group due to its proximity and function. However, anatomically, it stands apart. While the suboccipital muscles—rectus capitis posterior minor, obliquus capitis superior, and obliquus capitis inferior—originate from the posterior arch of the atlas (C1), the RCPM originates from the spinous process of the axis (C2). This distinction is crucial for clinicians and anatomists, as misidentification can lead to errors in treatment or analysis. For instance, in manual therapy, targeting the RCPM for suboccipital release may yield suboptimal results due to its different attachment point.
From a functional perspective, the RCPM plays a unique role in cervical stability. It assists in extending and rotating the head, particularly in movements involving the atlantoaxial joint. Unlike the suboccipital muscles, which primarily stabilize the occiput on the atlas, the RCPM’s attachment to the axis (C2) allows it to influence lower cervical mechanics. This makes it a key player in conditions like cervicogenic headaches or upper cervical dysfunction, where its dysfunction can mimic or exacerbate symptoms. Practitioners should note that stretching or strengthening exercises for the RCPM should be tailored to its distinct biomechanics, avoiding generic suboccipital protocols.
A comparative analysis highlights the RCPM’s anatomical and functional divergence. While the suboccipital muscles are innervated by the suboccipital nerve (C1), the RCPM is supplied by the dorsal ramus of C2. This neurological difference underscores its separate identity. Additionally, its longer line of pull from C2 to the occiput enables greater leverage in head extension, setting it apart from the shorter, more localized actions of the suboccipital group. For patients with chronic neck pain, differentiating between RCPM and suboccipital involvement can refine diagnostic accuracy and treatment efficacy.
Instructively, therapists and trainers can use this knowledge to design targeted interventions. For example, a patient with RCPM tightness might benefit from a supine chin tuck with a gentle nodding motion, emphasizing C2 extension. Conversely, suboccipital release techniques, such as a seated head tilt with overpressure, would focus on the atlas. Caution should be exercised in high-velocity manipulations, as the RCPM’s attachment to the axis makes it more susceptible to strain if misaligned during forceful movements. Age-related considerations are also important; older adults with degenerative changes at C2 may exhibit heightened RCPM stiffness, requiring gentler approaches.
Practically, understanding the RCPM’s unique role can improve outcomes in both clinical and fitness settings. For athletes, incorporating RCPM-specific exercises, such as resisted head extension with a band, can enhance cervical resilience. In yoga or Pilates, instructors should differentiate between cues for suboccipital and RCPM engagement to avoid compensatory patterns. For instance, in a prone cobra pose, emphasizing a gradual lift from the upper back rather than the head can isolate the RCPM effectively. This nuanced approach ensures that interventions address the muscle’s distinct anatomy and function, fostering better alignment and pain relief.
Bridge Exercise Benefits: Targeting Glutes, Core, and Lower Back Muscles
You may want to see also
Explore related products






![]()
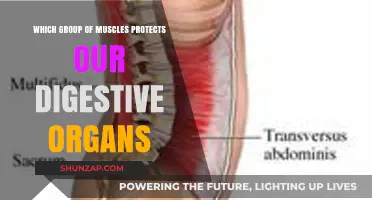
Rectus capitis posterior minor: Also not in the group, assists neck extension and rotation
The Rectus capitis posterior minor (RCPmi) is a small yet significant muscle that often flies under the radar in discussions about neck anatomy. Despite its name suggesting a posterior location, it does not belong to the suboccipital muscle group, which includes the obliquus capitis superior, obliquus capitis inferior, rectus capitis posterior major, and rectus capitis lateralis. Instead, the RCPmi is classified as a deep muscle of the neck, originating from the tubercle on the posterior arch of the atlas (C1) and inserting into the medial part of the inferior nuchal line of the occipital bone. This unique positioning allows it to play a distinct role in neck movement.
From a functional perspective, the RCPmi assists in neck extension and rotation, though its contribution is subtle compared to larger muscles like the trapezius or sternocleidomastoid. During neck extension, it works in conjunction with other deep muscles to stabilize the atlanto-occipital joint, which is crucial for maintaining proper head posture. In rotation, it helps tilt the head slightly, a movement often overlooked but essential for activities like checking blind spots while driving or glancing over a shoulder. For individuals experiencing neck stiffness or limited range of motion, targeted exercises that engage the RCPmi can provide relief. A simple exercise involves gently tilting the head backward while looking straight ahead, holding for 5–10 seconds, and repeating 10 times daily.
Comparatively, while the suboccipital muscles primarily focus on fine-tuning head movements and stabilizing the skull on the atlas, the RCPmi’s role is more specialized. Its attachment points and fiber orientation make it particularly effective in stabilizing the upper cervical spine during subtle movements. This distinction is vital for clinicians and anatomists, as misidentifying its function could lead to ineffective treatment strategies for neck pain or dysfunction. For instance, a patient with chronic neck stiffness might benefit from manual therapy targeting the RCPmi rather than the suboccipitals, highlighting the importance of precise anatomical knowledge.
Practically, incorporating RCPmi-focused stretches and strengthening exercises into a daily routine can improve neck mobility and reduce discomfort. A useful stretch involves sitting upright, placing one hand on the side of the head, and gently pulling the head toward the shoulder until a mild stretch is felt. Hold for 20–30 seconds and repeat on both sides. For strengthening, isometric exercises like pressing the back of the head into a wall or hand while maintaining a neutral spine can engage the RCPmi effectively. These exercises are particularly beneficial for office workers or individuals who spend long hours in fixed head positions, as they counteract the strain of prolonged postures.
In conclusion, while the Rectus capitis posterior minor may not be part of the suboccipital muscle group, its role in neck extension and rotation is indispensable. Understanding its unique anatomy and function allows for targeted interventions that enhance neck health and mobility. Whether through specific exercises or manual therapy, addressing the RCPmi can lead to significant improvements in both function and comfort, making it a muscle worth recognizing in the broader context of neck anatomy.
Daily Muscle Training: Benefits, Risks, and Recovery Explained
You may want to see also
Explore related products






![]()
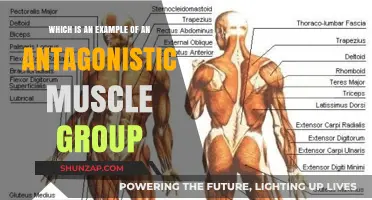
Obliquus capitis superior: Included in suboccipital group, extends and rotates head
The suboccipital muscle group is a collection of four muscles located at the base of the skull, crucial for fine movements and stability of the head. Among these, the obliquus capitis superior stands out for its unique role in extending and rotating the head. This muscle, originating from the transverse process of the atlas (C1) and inserting into the outer surface of the occipital bone, is often the focus of discussions about suboccipital function. However, it’s essential to clarify which muscles are not part of this group to avoid confusion in anatomical studies or therapeutic interventions.
From an analytical perspective, the obliquus capitis superior’s inclusion in the suboccipital group is straightforward due to its anatomical position and function. It works in tandem with the obliquus capitis inferior, rectus capitis posterior major, and rectus capitis posterior minor to control subtle head movements. For instance, during a rotation of the head, the obliquus capitis superior contracts on the opposite side to facilitate the motion. This specificity highlights why muscles like the trapezius or sternocleidomastoid, which act on the head but originate from different regions, are excluded from the suboccipital classification.
Instructively, understanding the obliquus capitis superior’s role is vital for physical therapists or chiropractors targeting suboccipital tension. Techniques such as soft tissue mobilization or dry needling can be applied to this muscle to alleviate pain or improve range of motion. For example, a patient with cervicogenic headaches may benefit from gentle stretching of the obliquus capitis superior, performed by tilting the head away from the affected side while applying light pressure. Caution must be taken to avoid overstretching, as this can exacerbate symptoms.
Comparatively, while the obliquus capitis superior is integral to the suboccipital group, its function contrasts with that of the rectus capitis posterior major, which primarily extends the head without significant rotation. This distinction is crucial in differential diagnosis, as pain localized to the obliquus capitis superior often presents with rotational limitations, whereas rectus capitis posterior major issues may manifest as stiffness during extension. Recognizing these differences ensures targeted treatment, whether through manual therapy or exercise prescription.
Descriptively, the obliquus capitis superior’s anatomy is both elegant and functional. Its oblique orientation allows it to contribute to both extension and rotation, making it a key player in activities like checking blind spots while driving or turning to engage in conversation. Despite its small size, its impact on cervical mechanics is profound, underscoring the importance of maintaining its health through regular stretching and strengthening exercises, such as chin tucks or resisted head rotations with a therapy band.
In conclusion, the obliquus capitis superior’s inclusion in the suboccipital group is defined by its anatomical location and functional role in extending and rotating the head. By distinguishing it from non-suboccipital muscles and understanding its unique contributions, practitioners can more effectively address cervical issues. Whether through targeted therapy or preventive exercises, appreciating this muscle’s specificity enhances both clinical outcomes and anatomical understanding.
Understanding Muscle Group Thickness: Factors, Variations, and Fitness Insights
You may want to see also
Explore related products





![]()
Obliquus capitis inferior: Part of the group, aids in head tilting and rotation
The suboccipital muscle group is a quartet of deep muscles at the base of the skull, crucial for fine movements of the head. Among them, the obliquus capitis inferior stands out for its unique role in head tilting and rotation. Unlike its counterparts, it originates from the spine of the axis (C2 vertebra) and inserts into the transverse process of the atlas (C1 vertebra), forming a distinct diagonal pathway. This anatomical arrangement allows it to contribute significantly to lateral flexion and rotation of the head, particularly when looking over one’s shoulder or tilting the ear toward the shoulder.
To understand its function, imagine you’re driving and need to check your blind spot. The obliquus capitis inferior is actively engaged as you tilt your head to the side and rotate it slightly. This movement is not just about flexibility but also stability, as the muscle helps maintain alignment between the first two cervical vertebrae during these motions. For individuals experiencing neck stiffness or pain, targeted exercises like gentle head tilts and rotations can help strengthen this muscle, improving both range of motion and comfort.
From a comparative perspective, the obliquus capitis inferior differs from other suboccipital muscles like the rectus capitis posterior major or minor, which primarily extend the head backward. Its diagonal orientation and attachment points make it uniquely suited for lateral movements, setting it apart in both structure and function. This specialization underscores its importance in activities requiring precise head control, such as sports or manual labor.
Practically, incorporating exercises to target the obliquus capitis inferior can be beneficial for anyone with a sedentary lifestyle or those recovering from neck injuries. Start with slow, controlled head tilts, holding each position for 5–10 seconds and repeating 10–15 times daily. Avoid abrupt movements, as these can strain the muscle. For added resistance, gently press your hand against the side of your head as you tilt, but only if it doesn’t cause pain. Consistency is key, as gradual strengthening will enhance both mobility and stability in the cervical spine.
In summary, the obliquus capitis inferior is a vital yet distinct member of the suboccipital muscle group, primarily responsible for head tilting and rotation. Its unique anatomy and function make it indispensable for everyday movements and specialized activities alike. By understanding its role and incorporating targeted exercises, individuals can improve neck health and prevent discomfort, ensuring this small but mighty muscle performs optimally.
Baseball Grip Strength: Key Hand Muscle Groups for Optimal Performance
You may want to see also
Explore related products





![]()
Semispinalis capitis: Not in suboccipital group, helps extend the head and neck
The suboccipital muscle group is a crucial set of muscles located at the base of the skull, playing a vital role in head and neck movements. However, not all muscles involved in these actions belong to this group. One such muscle is the semispinalis capitis, which, despite its significant function in extending the head and neck, is not classified as part of the suboccipital group. This distinction is essential for understanding the anatomy and mechanics of cervical movement.
From an anatomical perspective, the semispinalis capitis originates from the spinous processes of the upper thoracic and lower cervical vertebrae and inserts into the occipital bone. Its primary action is to extend the head and neck, working in conjunction with other muscles like the splenius capitis. Unlike the suboccipital muscles, which are located more inferiorly and have specific functions such as rotating and tilting the head, the semispinalis capitis operates over a broader range, contributing to more extensive movements. This differentiation highlights the importance of precise muscle categorization in both medical and therapeutic contexts.
For individuals experiencing neck pain or stiffness, understanding the role of the semispinalis capitis is crucial. Strengthening this muscle can improve posture and reduce strain on the cervical spine. Simple exercises like gentle head lifts while lying face down or using resistance bands to simulate extension can effectively target this muscle. However, it’s important to perform these exercises with caution, as overloading can lead to injury. Incorporating stretching routines for the opposing flexor muscles, such as the sternocleidomastoid, can also enhance balance and flexibility in the neck region.
Comparatively, while the suboccipital muscles are often addressed in treatments for conditions like cervicogenic headaches or occipital neuralgia, the semispinalis capitis is frequently overlooked. This muscle’s role in maintaining proper head alignment makes it a key player in preventing chronic neck issues. For instance, individuals who spend long hours at desks or looking at screens may develop tightness in this muscle, leading to discomfort. Regular breaks to stretch and strengthen the semispinalis capitis can mitigate these effects, offering a practical solution for modern lifestyle challenges.
In conclusion, the semispinalis capitis, though not part of the suboccipital group, is indispensable for head and neck extension. Its unique anatomical position and function necessitate targeted attention in both therapeutic and preventive care. By distinguishing it from the suboccipital muscles and incorporating specific exercises, individuals can achieve better cervical health and overall well-being. This nuanced understanding bridges the gap between anatomy and practical application, making it a valuable insight for anyone dealing with neck-related concerns.
Optimal Muscle Training Frequency for Women: A Comprehensive Guide
You may want to see also
Frequently asked questions
The trapezius muscle is not part of the suboccipital muscle group.
No, the sternocleidomastoid muscle is not part of the suboccipital muscle group.
No, the splenius capitis is not a member of the suboccipital muscle group.
No, the levator scapulae muscles are not part of the suboccipital muscle group.