The flexion of the 2nd to 5th distal phalanges, which allows the fingertips to bend toward the palm, is primarily caused by the flexor digitorum profundus muscle. This deep muscle originates from the upper half of the anterior and medial surfaces of the ulna, as well as the interosseous membrane, and its tendon passes through the carpal tunnel and divides into four slips, each inserting into the base of the distal phalanx of digits 2 through 5. The flexor digitorum profundus works in conjunction with the flexor digitorum superficialis, which flexes the middle phalanges, to achieve full finger flexion. Its action is crucial for gripping and manipulating objects, making it a key player in hand functionality.
| Characteristics | Values |
|---|---|
| Muscle Name | Flexor Digitorum Profundus |
| Origin | Ulna (medial epicondyle, anterior surface), interosseous membrane |
| Insertion | Distal phalanges of fingers 2-5 (flexor tendons) |
| Action | Flexion of distal interphalangeal joints (DIP) of fingers 2-5 |
| Nerve Supply | Ulnar nerve (C8-T1) for ulnar side (fingers 4 & 5), Median nerve (C7-T1) for radial side (fingers 2 & 3) |
| Artery Supply | Ulnar artery, radial artery |
| Antagonist Muscle | Extensor Digitorum |
| Function | Enables fine finger movements, gripping objects |
| Clinical Significance | Injuries to this muscle or its tendons can result in "mallet finger" or "Jersey finger" |
Explore related products






What You'll Learn
- Flexor Digitorum Profundus: Deep muscle, primary flexor of distal phalanges, originates from ulna, inserts on phalanges
- Muscle Origin and Insertion: Originates at ulna, inserts via tendons on distal phalanges of fingers 2-5
- Nerve Supply: Innervated by anterior interosseous nerve (C8, T1) from median nerve
- Function in Grip: Essential for fingertip flexion, crucial for gripping and holding objects firmly
- Clinical Relevance: Injury affects fine motor skills; treated via surgery or physical therapy for recovery
![]()
Flexor Digitorum Profundus: Deep muscle, primary flexor of distal phalanges, originates from ulna, inserts on phalanges
The Flexor Digitorum Profundus (FDP) is a deep muscle located in the forearm and is the primary flexor of the distal phalanges of the 2nd to 5th fingers. Its role is crucial in enabling fine motor skills, such as gripping objects or making a fist. The FDP originates from the upper three-quarters of the anterior (front) surface of the ulna, the medial aspect of the interosseous membrane, and the deep fascia of the forearm. This origin point provides a strong foundation for the muscle's function, allowing it to generate the force necessary for flexion.
Anatomically, the Flexor Digitorum Profundus is divided into four tendons, each corresponding to one of the fingers it acts upon: the index, middle, ring, and little fingers. These tendons pass through the carpal tunnel in the wrist and continue into the hand, where they travel within the flexor sheath. As they approach the distal phalanges, the tendons insert onto the base of each respective distal phalanx. This insertion point ensures that when the muscle contracts, it directly causes flexion at the distal interphalangeal (DIP) joints, allowing the fingertips to bend.
The FDP works in coordination with other muscles, particularly the Flexor Digitorum Superficialis (FDS), which flexes the middle phalanges. While the FDS is responsible for flexing the proximal interphalangeal (PIP) joints, the FDP acts independently to flex the DIP joints. This distinction is essential for precise finger movements, such as typing or playing a musical instrument. The deep location of the FDP beneath the FDS highlights its specialized role in controlling the most distal segment of the fingers.
Clinically, injuries to the Flexor Digitorum Profundus, such as tendon lacerations or ruptures, can significantly impair hand function. Given its deep position, repairing FDP injuries often requires surgical intervention to restore flexion at the DIP joints. Rehabilitation focuses on regaining strength and range of motion in the affected fingers. Understanding the FDP's anatomy and function is vital for diagnosing and treating such conditions effectively.
In summary, the Flexor Digitorum Profundus is a deep forearm muscle that originates from the ulna and inserts on the distal phalanges of the 2nd to 5th fingers. Its primary function is to flex the DIP joints, enabling precise fingertip movements. Its deep location, distinct from the FDS, underscores its unique role in hand mechanics. Knowledge of the FDP is essential for both anatomical understanding and clinical practice related to hand function and injuries.
Weak Calf Muscles: A Surprising Cause of Knee Pain
You may want to see also
Explore related products





![]()
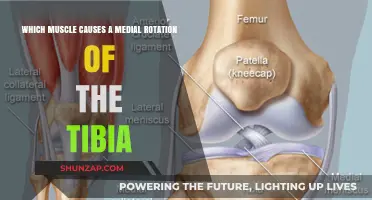
Muscle Origin and Insertion: Originates at ulna, inserts via tendons on distal phalanges of fingers 2-5
The muscle responsible for the flexion of the 2nd to 5th distal phalanges is the flexor digitorum profundus (FDP). This muscle plays a crucial role in finger movement, particularly in bending the fingertips toward the palm. Understanding its origin and insertion points is essential to grasp its function and anatomical significance. The FDP originates at the ulna, specifically along the anterior (front) and medial (inner) surfaces of the ulna bone in the forearm. This origin point provides a stable base for the muscle's action, allowing it to generate the necessary force for finger flexion.
From its origin at the ulna, the flexor digitorum profundus travels distally through the forearm, passing beneath the flexor digitorum superficialis (another finger flexor muscle). It then divides into four tendons, each of which inserts onto the distal phalanges of fingers 2-5 (index, middle, ring, and little fingers). These tendons are responsible for the precise movement of the fingertips, enabling actions such as gripping, typing, and manipulating objects. The insertion via tendons ensures a smooth and efficient transfer of force from the muscle to the bones of the fingers.
The insertion of the FDP tendons on the distal phalanges is facilitated by the flexor sheath and pulleys, which maintain proper tendon alignment and prevent bowstringing during flexion. This anatomical arrangement ensures that the muscle's contraction results in controlled and coordinated finger movements. The FDP's deep location in the forearm, as indicated by its name ("profundus" meaning deep), distinguishes it from the more superficial flexor digitorum superficialis, which primarily acts on the middle phalanges.
Clinically, the origin and insertion of the flexor digitorum profundus are critical in diagnosing and treating injuries such as tendon ruptures or conditions like trigger finger. Damage to the FDP tendons at their insertion points can significantly impair fine motor skills and hand function. Therefore, understanding the muscle's anatomical course from the ulna to the distal phalanges is vital for both anatomical study and medical practice.
In summary, the flexor digitorum profundus originates at the ulna and inserts via tendons on the distal phalanges of fingers 2-5, making it the primary muscle responsible for flexing the fingertips. Its precise origin and insertion points, along with its interaction with surrounding structures, ensure efficient and coordinated finger movements essential for daily activities.
Understanding the Root Causes of Bone and Muscle Pain
You may want to see also
Explore related products





![]()
Nerve Supply: Innervated by anterior interosseous nerve (C8, T1) from median nerve
The muscle responsible for the flexion of the 2nd to 5th distal phalanges is the flexor digitorum profundus (FDP). This muscle plays a crucial role in finger movement, particularly in bending the fingertips toward the palm. Understanding its nerve supply is essential for comprehending its function and clinical relevance. The flexor digitorum profundus is innervated by the anterior interosseous nerve, which originates from the median nerve, specifically the C8 and T1 nerve roots. This innervation is vital for the precise control of finger flexion, enabling actions such as gripping objects or making a fist.
The anterior interosseous nerve (AIN) is a branch of the median nerve that arises in the forearm. It supplies several muscles in the anterior compartment, including the FDP. The AIN’s role in innervating the FDP highlights its importance in fine motor skills and hand functionality. Damage to this nerve can result in impaired ability to flex the distal phalanges, significantly affecting daily activities. Therefore, the integrity of the AIN is critical for maintaining normal hand function.
The nerve supply from the C8 and T1 nerve roots ensures that the FDP receives adequate neural input for its function. These roots contribute to the formation of the median nerve, which then gives rise to the AIN. The C8 and T1 roots are part of the lower cervical and upper thoracic spinal segments, emphasizing the connection between spinal health and peripheral muscle function. Any compression or injury at these spinal levels can potentially disrupt the innervation of the FDP, leading to functional deficits in the hand.
Clinically, assessing the nerve supply of the FDP is crucial in diagnosing conditions such as anterior interosseous nerve syndrome or pronator teres syndrome, which can cause weakness in finger flexion. Electromyography (EMG) and nerve conduction studies are often used to evaluate the integrity of the AIN and its supply to the FDP. Understanding this innervation pattern aids in targeted treatment approaches, including physical therapy, surgical intervention, or nerve decompression, to restore optimal hand function.
In summary, the flexor digitorum profundus, which causes flexion of the 2nd to 5th distal phalanges, is innervated by the anterior interosseous nerve (C8, T1) from the median nerve. This specific nerve supply is fundamental to the muscle’s ability to perform precise finger movements. Recognizing the anatomical and clinical significance of this innervation is essential for diagnosing and managing conditions that affect hand functionality.
Muscle Soreness: Activities That Cause Delayed Onset Pain
You may want to see also
Explore related products






![]()
Function in Grip: Essential for fingertip flexion, crucial for gripping and holding objects firmly
The muscle primarily responsible for the flexion of the 2nd to 5th distal phalanges is the flexor digitorum profundus (FDP). This muscle plays a pivotal role in hand functionality, particularly in the context of grip strength and precision. When discussing its function in grip, the FDP is indispensable for fingertip flexion, a movement essential for securely gripping and holding objects. This action allows the fingertips to curl around items, ensuring a firm and controlled grasp. Without the FDP, tasks requiring fine motor skills and strong grip strength, such as writing, typing, or lifting objects, would be significantly impaired.
In the mechanics of grip, the FDP works in tandem with other muscles, but its role is uniquely critical for distal phalange flexion. When you attempt to hold an object, the FDP contracts, pulling on the tendons that connect to the distal phalanges of the 2nd to 5th fingers. This contraction enables the fingertips to bend, creating a concave surface that conforms to the shape of the object being held. This conformity is key to maintaining a stable grip, as it maximizes the contact area between the fingers and the object, distributing pressure evenly and preventing slippage.
The importance of the FDP in daily activities cannot be overstated. For instance, when holding a pen, the FDP ensures that the fingertips apply the necessary pressure to control the writing instrument without crushing it. Similarly, in tasks like opening a jar or carrying a heavy bag, the FDP provides the fingertip flexion required to maintain a secure hold, even when the object is slippery or awkwardly shaped. Its ability to generate precise and powerful flexion movements makes it a cornerstone of hand functionality in both mundane and complex tasks.
Moreover, the FDP's role extends beyond static grip strength; it is equally vital for dynamic gripping actions. When manipulating objects, such as turning a doorknob or playing a musical instrument, the FDP enables the fingertips to adjust their flexion continuously. This adaptability ensures that the grip remains firm yet flexible, allowing for smooth transitions between different hand positions. Without this dynamic capability, tasks requiring dexterity and coordination would be far more challenging, if not impossible.
In summary, the flexor digitorum profundus is essential for fingertip flexion, a function that underpins the ability to grip and hold objects firmly. Its role in both static and dynamic gripping actions highlights its significance in everyday hand use. Whether performing tasks that require precision, strength, or adaptability, the FDP ensures that the distal phalanges of the 2nd to 5th fingers contribute effectively to a secure and controlled grip. Understanding its function not only sheds light on the complexity of hand anatomy but also emphasizes the importance of maintaining its health for optimal hand functionality.
Magnesium Deficiency: The Link to Muscle Spasms
You may want to see also
Explore related products






![]()
Clinical Relevance: Injury affects fine motor skills; treated via surgery or physical therapy for recovery
The flexion of the 2nd to 5th distal phalanges is primarily controlled by the flexor digitorum profundus (FDP) muscle. This muscle originates from the upper half of the anterior and medial surfaces of the ulna, the interosseous membrane, and the upper half of the anterior surface of the radius. Its tendons pass through the carpal tunnel and along the palm, eventually inserting into the distal phalanges of the index, middle, ring, and little fingers. Injury to the FDP or its associated structures can significantly impair fine motor skills, as these movements are essential for tasks requiring precision, such as writing, typing, or grasping small objects.
Clinical Relevance: Injury affects fine motor skills
Injuries to the FDP or its tendons, such as lacerations, ruptures, or tendonitis, can severely disrupt hand function. For instance, a Jersey finger (rupture of the FDP tendon at its distal insertion) or a flexor tendon laceration in the palm or forearm can lead to an inability to flex the distal phalanges. This loss of flexion directly impacts fine motor skills, as patients may struggle with activities requiring fingertip control. Even partial injuries can result in weakness, stiffness, or pain, further limiting hand dexterity. Early diagnosis and intervention are critical to prevent long-term disability and ensure optimal recovery.
Surgical Treatment for FDP Injuries
Surgery is often the primary treatment for severe FDP injuries, such as complete tendon ruptures or complex lacerations. Procedures like primary tendon repair involve suturing the torn ends of the tendon, while tendon grafting may be necessary if there is significant tissue loss. Postoperative care is crucial, as improper healing can lead to adhesions, which restrict tendon gliding and impair finger movement. Surgeons may use techniques like early protected mobilization or dynamic splinting to promote healing while preventing stiffness. Rehabilitation following surgery is a gradual process, often spanning several months, to restore strength, flexibility, and function.
Physical Therapy for Recovery
Physical therapy plays a pivotal role in both nonsurgical and postoperative management of FDP injuries. Therapists design individualized programs to improve range of motion, reduce stiffness, and strengthen the hand and forearm muscles. Techniques such as passive and active stretching, tendon gliding exercises, and grip strengthening are commonly employed. For patients with adhesions or scar tissue, manual therapy and instrument-assisted soft tissue mobilization can help restore tendon mobility. Additionally, modalities like heat, cold, or ultrasound therapy may be used to alleviate pain and inflammation. Consistent adherence to a therapy regimen is essential for regaining fine motor skills and returning to daily activities.
Prevention and Long-Term Management
Preventing FDP injuries involves protective measures, such as wearing gloves or guards during high-risk activities like sports or manual labor. For individuals with repetitive strain or overuse, ergonomic adjustments and regular hand exercises can reduce the risk of tendonitis or ruptures. Long-term management focuses on maintaining hand health through ongoing exercise, monitoring for recurrent symptoms, and addressing any functional limitations. Patient education is key, as understanding the importance of proper healing and rehabilitation can significantly improve outcomes. By combining surgical intervention, physical therapy, and preventive strategies, clinicians can help patients recover fine motor skills and restore hand functionality after FDP injuries.
Salt, Muscle Cramps, and You
You may want to see also
Frequently asked questions
The flexor digitorum profundus (FDP) muscle is the primary muscle responsible for the flexion of the 2nd to 5th distal phalanges.
The flexor digitorum profundus muscle attaches to the distal phalanges via tendons that pass through the flexor sheath and insert into the base of the distal phalanges of the 2nd to 5th fingers.
Yes, the flexor digitorum superficialis (FDS) muscle also assists in the flexion of the 2nd to 5th distal phalanges, although its primary action is to flex the middle phalanges.
The flexor digitorum profundus muscle is innervated by the ulnar nerve (C8-T1) for the 4th and 5th fingers, and by the median nerve (C7-C8) for the 2nd and 3rd fingers.