The transversospinalis group, a deep muscle layer of the back, plays a crucial role in spinal stability and movement. Among its components, the semispinalis capitis stands out as the only muscle in this group that attaches to the cranium. Originating from the cervical and upper thoracic vertebrae, it ascends to insert on the occipital bone, specifically at the external occipital protuberance and the superior nuchal line. This unique attachment allows the semispinalis capitis to contribute to head extension and stabilization, distinguishing it from other transversospinalis muscles that primarily act on the spine. Its cranial connection highlights its importance in both posture and cervical function.
Explore related products






What You'll Learn
![]()
Semispinalis capitis origin and insertion
The semispinalis capitis is a unique muscle within the transversospinalis group, distinguished by its attachment to the cranium. Unlike its counterparts that primarily connect vertebrae, this muscle bridges the cervical and thoracic spine to the occipital bone, playing a pivotal role in head extension and stability. Understanding its origin and insertion points is essential for clinicians, anatomists, and anyone seeking to address neck pain or improve posture.
Anatomical Foundations: Origin and Insertion
The semispinalis capitis originates from the spinous processes of the upper thoracic (T6–T12) and lower cervical (C6–C7) vertebrae. These multiple attachment points create a broad, fan-like structure that converges as the muscle ascends. Its insertion is precise: the muscle fibers attach to the lateral aspect of the occipital bone, specifically the superior nuchal line, a bony ridge located at the base of the skull. This cranial connection sets it apart from other transversospinalis muscles, which typically insert on vertebral structures.
Functional Implications
The semispinalis capitis acts as a primary extender of the head, working in concert with other suboccipital and neck muscles to tilt the face upward. For example, when looking up at a shelf or during exercises like cervical extension stretches, this muscle is actively engaged. However, its deep location and proximity to sensitive neural structures mean overuse or strain can contribute to chronic neck pain or headaches. Clinicians often target this muscle in manual therapy or prescribe specific stretches to alleviate tension.
Practical Tips for Engagement and Care
To strengthen the semispinalis capitis, incorporate controlled head extension exercises, such as lying face down and gently lifting the chin toward the ceiling. Hold for 5–10 seconds, repeating 10–15 times daily. For relief, apply a warm compress to the upper back and base of the skull, followed by gentle self-massage along the muscle’s path. Avoid abrupt or forceful movements, as these can strain the muscle or irritate nearby nerves. Individuals with pre-existing neck conditions should consult a physical therapist before starting new exercises.
Clinical Relevance and Takeaway
Knowledge of the semispinalis capitis’s origin and insertion is invaluable for diagnosing and treating neck-related issues. Its unique cranial attachment makes it a key player in both posture and pain syndromes. By understanding its anatomy and function, practitioners can design targeted interventions, while individuals can adopt preventive measures to maintain neck health. Whether in rehabilitation or daily life, this muscle’s role underscores the intricate interplay between spinal and cranial structures.
Effective Muscle Group Workouts: Strategies for Balanced Strength Training
You may want to see also
Explore related products




![]()
Semispinalis capitis function in head posture
The semispinalis capitis, a muscle of the transversospinalis group, plays a crucial role in maintaining and adjusting head posture. Originating from the cervical and upper thoracic vertebrae, it inserts directly onto the occipital bone of the cranium. This unique attachment point allows it to act as a primary stabilizer and mover of the head, particularly in extension and rotation. Understanding its function is essential for addressing posture-related issues and preventing strain in the neck and upper back.
From an anatomical perspective, the semispinalis capitis works in conjunction with other muscles to counteract the forward pull of gravity on the head. When activated, it helps lift the head backward (extension) and assists in turning it side to side (rotation). This muscle is particularly active during activities like looking upward, such as when reading from a screen mounted above eye level or gazing at the sky. Overuse or imbalance in this muscle can lead to chronic neck pain, making it a key focus in ergonomic assessments and physical therapy interventions.
To optimize the function of the semispinalis capitis, consider incorporating targeted exercises into your routine. For instance, gentle head retraction exercises, where you pull your head straight back while keeping your chin level, can strengthen this muscle without straining it. Hold the position for 5–10 seconds and repeat 10–15 times daily. Avoid jerking movements or excessive force, as these can exacerbate tension rather than alleviate it. Pairing these exercises with stretches for the chest and front of the neck can further promote balanced posture.
A comparative analysis reveals that while the semispinalis capitis is vital for head extension, it often works in tandem with the splenius capitis and longissimus capitis muscles. However, its direct attachment to the cranium gives it a unique role in fine-tuning head position. For individuals who spend long hours at desks or on devices, this muscle can become overworked, leading to tightness and discomfort. Regular breaks to reset posture, coupled with mindful activation of the semispinalis capitis, can mitigate these effects.
In practical terms, maintaining proper head posture isn’t just about muscle function—it’s about habit. For example, adjusting your screen to eye level reduces the need for the semispinalis capitis to work overtime. Similarly, using a headset for phone calls prevents craning the neck, which can strain this muscle. For older adults or those with degenerative spinal conditions, gentle yoga or Pilates routines can improve flexibility and strength in this area without causing injury. By prioritizing awareness and consistency, you can ensure the semispinalis capitis supports your posture effectively throughout daily activities.
Full-Body Home Workouts: Target All Muscle Groups with Resistance Bands
You may want to see also
Explore related products






![]()
Nerve supply to Semispinalis capitis
The semispinalis capitis, a muscle of the transversospinalis group, uniquely attaches to the cranium, distinguishing it from other muscles in this category. Its nerve supply is a critical aspect of its function, as it ensures proper innervation for movement and stability of the head and neck. Understanding this nerve supply is essential for clinicians, anatomists, and anyone interested in the biomechanics of the cervical and thoracic regions.
From an anatomical perspective, the semispinalis capitis is primarily innervated by the posterior branches of the cervical nerves, specifically C1 to C5. These nerves arise from the cervical plexus and travel alongside the muscle fibers to provide motor control. The precise distribution of these nerves ensures that the muscle can contract efficiently to extend and rotate the head, particularly during movements like looking upward or turning the head side to side. This innervation pattern highlights the muscle’s role in fine-tuning cervical and cranial positioning.
Clinically, knowledge of the nerve supply to the semispinalis capitis is invaluable for diagnosing and treating conditions such as cervicalgia or whiplash injuries. For instance, nerve root compression at levels C3 to C5 can lead to weakened or impaired function of this muscle, resulting in reduced head stability or chronic pain. Practitioners may use this information to guide targeted therapies, such as nerve blocks or physical rehabilitation exercises, to restore function. Patients experiencing neck stiffness or headaches may benefit from exercises that specifically engage the semispinalis capitis, such as gentle neck extensions or isometric holds, performed under professional guidance.
A comparative analysis reveals that while the semispinalis capitis shares its nerve supply with other muscles in the transversospinalis group, its attachment to the cranium makes it uniquely susceptible to strain in activities involving prolonged head positioning, such as desk work or smartphone use. Unlike its counterparts, which primarily stabilize the thoracic spine, the semispinalis capitis must counteract gravitational forces acting on the head, placing greater demand on its neural input. This distinction underscores the importance of ergonomic adjustments and regular stretching to prevent overuse injuries.
In practical terms, individuals can support the health of the semispinalis capitis and its nerve supply through simple measures. Incorporating neck stretches into daily routines, such as gently tilting the head ear-to-shoulder, can relieve tension. Maintaining proper posture, especially during screen use, reduces unnecessary strain on the muscle and its innervation. For those with persistent symptoms, consulting a healthcare provider for a nerve conduction study or electromyography can help identify underlying issues related to the cervical nerve roots. By addressing both muscle and nerve health, one can optimize the function of the semispinalis capitis and maintain overall cervical well-being.
Mastering Movement: Understanding Your Body's Major Muscle Groups
You may want to see also
Explore related products






![]()
Clinical relevance of Semispinalis capitis
The semispinalis capitis, a muscle of the transversospinalis group, uniquely attaches to the cranium, specifically the occipital bone. This anatomical distinction grants it a pivotal role in cervical stability and head posture, making it clinically significant in various musculoskeletal conditions.
Understanding its function and associated pathologies is crucial for accurate diagnosis and effective treatment.
Identifying Semispinalis Capitis Dysfunction: A Clinical Perspective
Imagine a patient presenting with chronic neck pain, headaches originating at the base of the skull, and restricted cervical extension. Upon palpation, tenderness is noted along the nuchal line, particularly at the insertion point of the semispinalis capitis. This clinical picture strongly suggests myofascial trigger points within the muscle, a common source of cervicogenic headaches and neck pain. Trigger point injections, dry needling, or targeted massage therapy can provide significant relief by releasing these hyperirritable spots.
Studies have shown that trigger point injections with a local anesthetic and corticosteroid combination can offer pain reduction for several weeks, allowing for concurrent physical therapy to address underlying postural imbalances and muscle weakness.
Beyond Trigger Points: The Semispinalis Capitis in Cervical Instability
While trigger points are a frequent culprit, semispinalis capitis dysfunction can also contribute to cervical instability, particularly in cases of trauma or degenerative conditions. This muscle plays a crucial role in resisting excessive flexion and lateral bending of the cervical spine. Weakness or atrophy of the semispinalis capitis can lead to increased segmental motion, potentially causing nerve compression, disc herniation, or even spinal cord compromise.
Rehabilitation Strategies: Strengthening the Semispinalis Capitis
Rehabilitation programs targeting the semispinalis capitis are essential for restoring cervical stability and preventing recurrent pain. Isometric exercises like head retraction against resistance (e.g., using a resistance band or therapist's hand) effectively activate this muscle. Progressive strengthening can be achieved by incorporating dynamic exercises like prone cobra holds or cervical extension against gravity. It's crucial to start with low resistance and gradually increase intensity to avoid exacerbating existing pain.
A Multifaceted Approach to Clinical Management
Addressing semispinalis capitis dysfunction requires a comprehensive approach. Accurate diagnosis through thorough history, physical examination, and potentially imaging studies is paramount. Treatment modalities may include manual therapy, trigger point interventions, and targeted exercise programs. Patient education on posture, ergonomics, and self-management techniques is vital for long-term success. By recognizing the clinical relevance of the semispinalis capitis, healthcare professionals can effectively manage a range of cervical spine conditions and improve patient outcomes.
Daily Muscle Rotation: Effective or Overkill for Your Workout Routine?
You may want to see also
Explore related products






![]()
Differentiation from other cranial muscles
The muscle of the transversospinalis group that attaches to the cranium is the rectus capitis posterior minor (RCPmi). This small yet significant muscle originates from the tubercle on the posterior arch of the atlas (C1) and inserts onto the occipital bone, specifically the medial part of the inferior nuchal line. Its cranial attachment sets it apart from other muscles in the group, which typically span between vertebrae rather than connecting to the skull. This unique feature necessitates a clear differentiation from other cranial muscles, both in structure and function.
Anatomical Distinction: Unlike superficial cranial muscles such as the splenius capitis or sternocleidomastoid, which primarily move the head and neck in large, visible ranges, the RCPmi is deep and operates in a more localized, stabilizing role. Its attachment to the occipital bone and atlas positions it as a key player in fine, rotational movements of the head, particularly in extension and ipsilateral rotation. This contrasts with the broader actions of the temporalis or masseter, which are involved in jaw movement rather than cervical stabilization.
Functional Specialization: The RCPmi’s role in stabilizing the atlanto-occipital joint differentiates it from muscles like the obliquus capitis superior and obliquus capitis inferior, which also attach to the atlas but focus on lateral flexion and rotation. While these muscles work in tandem with the RCPmi, their actions are more lateralized, whereas the RCPmi’s primary function is to resist excessive flexion and maintain alignment between the skull and cervical spine. This specialization is critical in preventing strain during subtle head movements, such as nodding or turning the head to check blind spots while driving.
Clinical Relevance: Understanding the RCPmi’s unique cranial attachment is essential in diagnosing and treating cervicogenic headaches or upper cervical instability. Unlike the trapezius or semispinalis capitis, which can refer pain more diffusely, dysfunction in the RCPmi often presents as localized pain at the base of the skull. Practitioners can differentiate RCPmi involvement by palpating the suboccipital region and assessing pain during resisted extension. Stretching this muscle involves gentle chin tucks, holding for 20–30 seconds, repeated 3–4 times daily, while avoiding over-extension exercises that may exacerbate strain.
Practical Application: For individuals experiencing chronic neck stiffness, isolating the RCPmi in exercises can provide targeted relief. A simple technique is to lie supine with a small towel roll under the neck, gently pressing the head into the towel to engage the suboccipital muscles without straining. This contrasts with general neck stretches, which often target larger muscles like the levator scapulae or scalenes. By focusing on the RCPmi, patients can address the root cause of cranial-cervical misalignment, reducing the risk of recurring discomfort.
Optimal Rest Days: Timing Your Workouts for Maximum Muscle Growth
You may want to see also
Frequently asked questions
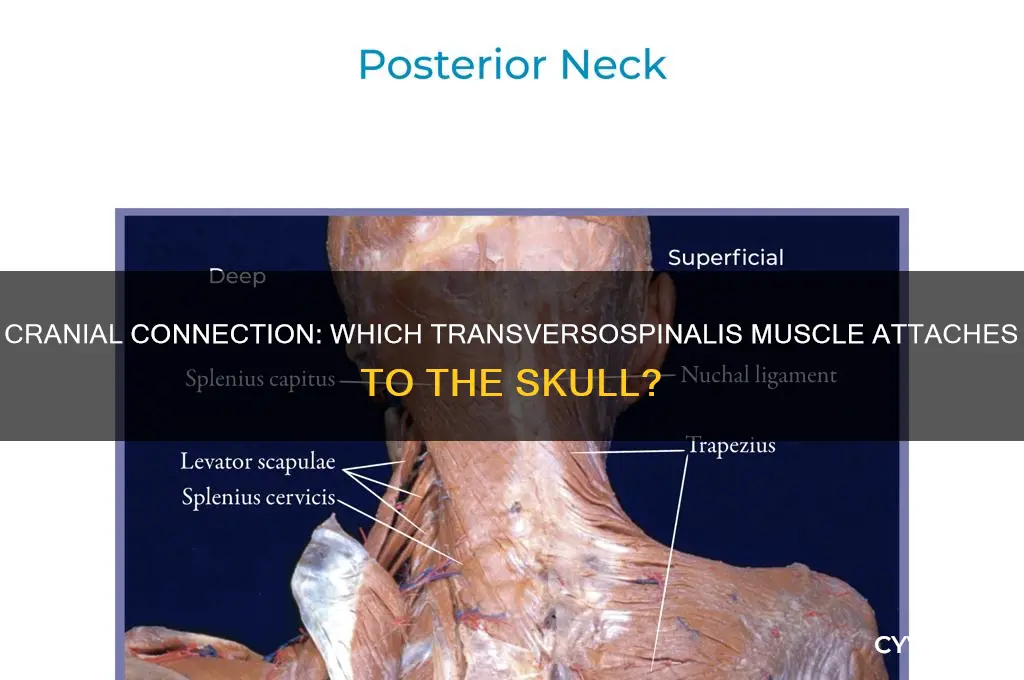
The splenius capitis is the muscle of the transversospinalis group that attaches to the cranium, specifically at the mastoid process and the nuchal ridge.
Yes, the splenius capitis is classified as part of the transversospinalis group, which also includes the semispinalis and multifidus muscles.
The splenius capitis, which attaches to the cranium, primarily functions to extend, laterally flex, and rotate the head and neck.