Muscle relaxants are commonly used in clinical settings to treat conditions such as muscle spasms, stiffness, and pain, but some of these medications can trigger histamine release, leading to adverse effects such as itching, flushing, or allergic reactions. Histamine release is particularly associated with certain neuromuscular blocking agents used in anesthesia, such as succinylcholine and mivacurium, which can cause dose-dependent histamine liberation from mast cells. Additionally, some centrally acting muscle relaxants, like cyclobenzaprine, may indirectly influence histamine pathways, though their primary mechanism does not involve direct histamine release. Understanding which muscle relaxants cause histamine release is crucial for clinicians to minimize side effects and ensure patient safety, especially in individuals with a history of allergies or mast cell disorders.
Explore related products






What You'll Learn
![]()
Mechanism of Histamine Release
Muscle relaxants are commonly used in anesthesia and intensive care to facilitate endotracheal intubation and provide skeletal muscle relaxation during surgical procedures. However, certain muscle relaxants are known to cause histamine release, which can lead to adverse effects such as hypotension, flushing, and bronchospasm. The mechanism of histamine release involves the interaction of these muscle relaxants with specific receptors or cells in the body, primarily mast cells and basophils, which are rich in histamine granules. Understanding this mechanism is crucial for clinicians to anticipate and manage potential side effects.
The primary mechanism of histamine release by muscle relaxants involves the activation of mast cells and basophils. These cells contain histamine in their granules and release it upon stimulation. Muscle relaxants like succinylcholine and decamethonium are known to directly stimulate the release of histamine from these cells. Succinylcholine, for instance, acts by depolarizing the plasma membrane of skeletal muscle fibers, but it also interacts with mast cells, leading to their degranulation. This process is mediated by the activation of voltage-gated channels on mast cells, which triggers the exocytosis of histamine-containing granules into the extracellular space.
Another pathway involves the interaction of muscle relaxants with immunoglobulin E (IgE) receptors on mast cells and basophils. While this mechanism is less direct, certain muscle relaxants may act as haptens, binding to proteins and forming complexes that cross-link IgE antibodies. This cross-linking initiates a signaling cascade, leading to the activation of mast cells and subsequent histamine release. Although this mechanism is not the primary cause of histamine release by muscle relaxants, it highlights the complexity of interactions between these drugs and the immune system.
Additionally, some muscle relaxants may indirectly cause histamine release by inducing the complement system or activating other inflammatory pathways. For example, the activation of the complement cascade can lead to the generation of anaphylatoxins (C3a and C5a), which are potent stimulators of mast cells and basophils. While this mechanism is less common with muscle relaxants, it underscores the potential for indirect histamine release through systemic inflammatory responses.
In summary, the mechanism of histamine release by muscle relaxants primarily involves the direct stimulation of mast cells and basophils, leading to their degranulation. Drugs like succinylcholine activate voltage-gated channels on these cells, triggering the release of histamine. Secondary mechanisms, such as IgE receptor cross-linking or complement system activation, may also contribute, though to a lesser extent. Clinicians must be aware of these mechanisms to manage histamine-related side effects effectively, particularly in patients with a predisposition to allergic or anaphylactic reactions.
Nicotine and Muscle Cramps: Is There a Link?
You may want to see also
Explore related products






![]()
Muscle Relaxants Linked to Histamine
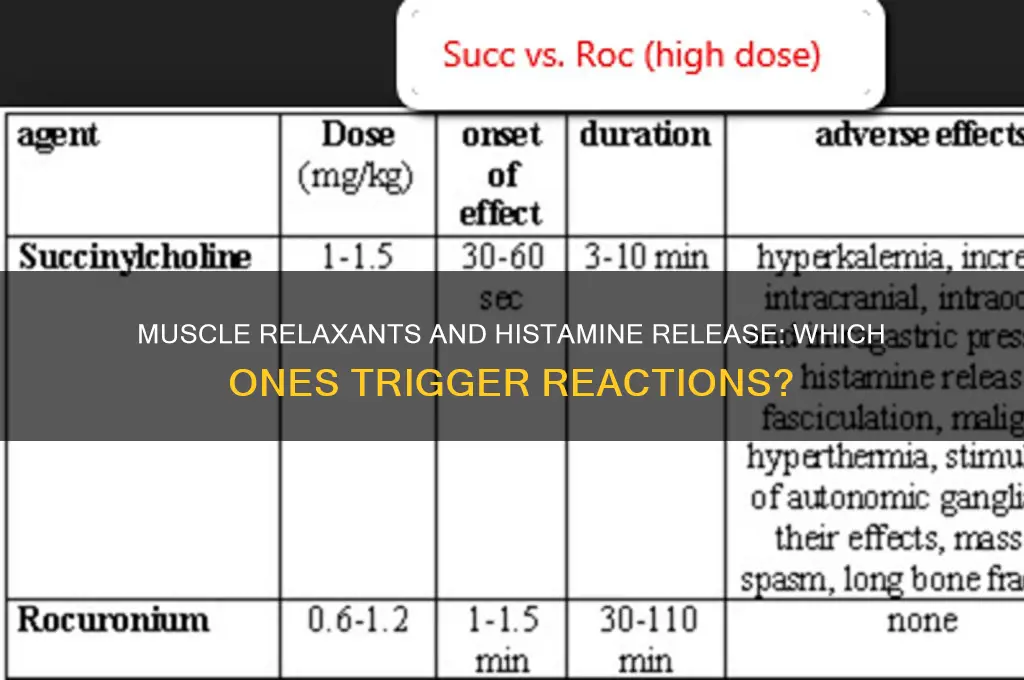
Muscle relaxants are commonly prescribed to alleviate muscle spasms and pain, but some of these medications have been linked to histamine release, which can lead to adverse effects such as itching, flushing, and allergic reactions. Histamine is a compound involved in immune responses and is released by mast cells in response to certain triggers. Among muscle relaxants, succinylcholine, a depolarizing neuromuscular blocking agent, is well-documented to cause histamine release. This occurs due to its mechanism of action, which involves stimulating muscle cells and subsequently triggering mast cell degranulation. Patients receiving succinylcholine may experience symptoms like skin flushing, bronchospasm, or hypotension, particularly if they are sensitive to histamine or have pre-existing conditions like asthma.
Another muscle relaxant associated with histamine release is meprobamate, a centrally acting agent used for its anxiolytic and muscle relaxant properties. Meprobamate has been reported to induce histamine-mediated reactions in some individuals, though the exact mechanism is not fully understood. These reactions can manifest as rashes, itching, or more severe allergic responses. It is important for healthcare providers to monitor patients closely when prescribing meprobamate, especially those with a history of allergies or hypersensitivity.
In addition to these, certain non-depolarizing neuromuscular blocking agents, such as atracurium and mivacurium, have also been implicated in histamine release. Atracurium, for instance, is known to cause histamine-mediated cardiovascular effects, including hypotension and tachycardia, particularly during rapid intravenous administration. Mivacurium, though less commonly used today, has a higher propensity to release histamine compared to other neuromuscular blockers, often leading to flushing and hypotension. These effects are dose-dependent and more pronounced in susceptible individuals.
It is crucial for clinicians to be aware of these associations when prescribing muscle relaxants, especially in patients with a history of histamine-related conditions or allergies. Alternatives with lower histamine-releasing potential, such as rocuronium or vecuronium, may be considered in high-risk patients. Additionally, premedication with antihistamines or other prophylactic measures can be employed to mitigate the risk of adverse reactions. Understanding the link between muscle relaxants and histamine release is essential for safe and effective patient management.
Patients should also be educated about the potential symptoms of histamine release, such as itching, flushing, or difficulty breathing, and advised to seek immediate medical attention if these occur. While muscle relaxants are valuable therapeutic tools, their histamine-releasing properties underscore the importance of individualized treatment plans and vigilant monitoring. By staying informed and proactive, healthcare providers can minimize risks and optimize outcomes for patients requiring muscle relaxant therapy.
Understanding Shin Muscle Spasms: Causes and Prevention Tips
You may want to see also
Explore related products






![]()
Clinical Symptoms of Histamine Release
Muscle relaxants are commonly used in anesthesia and intensive care to facilitate endotracheal intubation and provide skeletal muscle relaxation during surgical procedures. However, certain muscle relaxants, such as succinylcholine and mivacurium, are known to cause histamine release, which can lead to a range of clinical symptoms. Histamine release occurs due to the activation of mast cells and basophils, resulting in the discharge of preformed mediators, including histamine, into the systemic circulation. Understanding the clinical symptoms of histamine release is crucial for prompt recognition and management of these adverse effects.
The clinical symptoms of histamine release typically manifest within minutes of administering the offending muscle relaxant. One of the most immediate and common symptoms is cutaneous flushing, characterized by a sudden, transient redness and warmth of the skin, particularly in the upper body and face. This occurs due to the vasodilatory effects of histamine on blood vessels. Patients may also experience pruritus, or intense itching, which can be localized or generalized. These symptoms are often mild but can be distressing and may require intervention to alleviate discomfort.
Another significant clinical manifestation is bronchospasm, which poses a serious risk, especially in patients with pre-existing respiratory conditions such as asthma. Histamine-induced bronchospasm results from the contraction of smooth muscles in the airways, leading to wheezing, shortness of breath, and increased airway resistance. This can compromise ventilation and oxygenation, necessitating immediate medical attention. Clinicians should be prepared to administer bronchodilators or other supportive measures to manage this potentially life-threatening complication.
Hypotension is another critical symptom of histamine release, arising from systemic vasodilation and decreased vascular resistance. This can lead to a rapid drop in blood pressure, which may be accompanied by tachycardia as the body attempts to compensate. Severe hypotension can impair organ perfusion and requires prompt intervention, such as fluid resuscitation or vasopressor support. Monitoring hemodynamic parameters closely during the administration of muscle relaxants known to cause histamine release is essential to detect and manage this complication effectively.
In some cases, histamine release can trigger anaphylaxis, a severe, life-threatening allergic reaction. Symptoms of anaphylaxis include a combination of cutaneous, respiratory, and cardiovascular manifestations, such as generalized flushing, angioedema, stridor, bronchospasm, hypotension, and collapse. Anaphylaxis requires immediate recognition and treatment, including the administration of epinephrine, antihistamines, and corticosteroids, along with supportive care to stabilize the patient. Awareness of the potential for anaphylaxis with certain muscle relaxants is critical for patient safety.
Lastly, tachycardia and headache may also occur as part of the histamine release syndrome. Tachycardia is often a compensatory response to hypotension, while headaches can result from histamine-induced vasodilation. Although these symptoms are generally less severe than bronchospasm or hypotension, they contribute to the overall clinical picture and should not be overlooked. Clinicians must remain vigilant and consider the possibility of histamine release when administering muscle relaxants like succinylcholine or mivacurium, ensuring appropriate monitoring and preparedness to manage these symptoms effectively.
Muscle Strain: Back Pain Leading to Chest Discomfort
You may want to see also
Explore related products





![]()
High-Risk Patient Populations
Patients with a history of allergic or hypersensitivity reactions are at significantly elevated risk when prescribed muscle relaxants known to cause histamine release. Muscle relaxants such as succinylcholine and mivacurium are well-documented to trigger histamine release, which can lead to symptoms ranging from mild pruritus to severe anaphylaxis. Individuals with a personal or family history of allergies, asthma, or atopic conditions are particularly vulnerable. Clinicians must carefully review patient histories and consider alternative agents to avoid potentially life-threatening reactions in this population.
Patients with cardiovascular instability represent another high-risk group. Histamine release induced by certain muscle relaxants can cause vasodilation, hypotension, and tachycardia, exacerbating existing cardiovascular conditions. Patients with hypertension, coronary artery disease, or heart failure may experience worsened hemodynamic instability when exposed to these agents. Additionally, elderly patients, who often have comorbid cardiovascular issues, are at heightened risk due to age-related physiological changes and reduced compensatory mechanisms. Close monitoring and cautious dosing are essential in these cases.
Pediatric and geriatric populations require special consideration due to their unique physiological vulnerabilities. Children, particularly infants and young children, have immature metabolic and excretory systems, making them more susceptible to adverse effects from histamine-releasing muscle relaxants. Similarly, elderly patients often have diminished renal and hepatic function, which can prolong drug half-lives and increase the risk of accumulation and toxicity. Both age groups may also have limited ability to communicate symptoms, necessitating vigilant observation during and after administration of these medications.
Patients with renal or hepatic impairment are at increased risk due to altered drug metabolism and elimination. Muscle relaxants that cause histamine release are often metabolized by the liver or excreted by the kidneys. Impaired organ function can lead to drug accumulation, prolonging exposure and increasing the likelihood of histamine-mediated adverse effects. Clinicians should adjust dosages or select alternative agents with caution in these patients, ensuring therapeutic goals are met without compromising safety.
Individuals with mast cell disorders, such as mastocytosis or mast cell activation syndrome (MCAS), are uniquely vulnerable to muscle relaxants that induce histamine release. These conditions predispose patients to excessive histamine release even in response to minimal triggers, significantly amplifying the risk of severe reactions. Symptoms such as flushing, hypotension, bronchospasm, and anaphylaxis can occur rapidly and require immediate intervention. Identifying these patients prior to administration and having emergency protocols in place is critical to managing their care safely.
In all high-risk populations, proactive risk assessment and individualized treatment planning are essential. Clinicians should weigh the benefits of muscle relaxants against the potential risks, consider alternative agents when possible, and ensure appropriate monitoring and resuscitative measures are available. Patient education and informed consent are also vital, particularly in those with known predisposing conditions, to foster shared decision-making and improve outcomes.
Lyme Disease: Understanding Muscle Loss and Recovery
You may want to see also
Explore related products






![]()
Alternatives to Histamine-Releasing Relaxants
When considering alternatives to muscle relaxants that cause histamine release, it's essential to identify medications that provide effective muscle relaxation without triggering histamine-related side effects such as itching, flushing, or allergic reactions. One prominent class of muscle relaxants known to release histamine includes succinylcholine, a depolarizing neuromuscular blocker commonly used in anesthesia. For patients sensitive to histamine release, non-depolarizing neuromuscular blockers like rocuronium or vecuronium are viable alternatives. These agents do not stimulate histamine release and are widely used in surgical settings for their predictable and reversible muscle relaxation properties.
Another alternative to histamine-releasing relaxants is the use of centrally acting muscle relaxants, which work by inhibiting neuronal activity in the central nervous system rather than directly affecting muscle fibers. Medications such as cyclobenzaprine, tizanidine, and baclofen fall into this category. These drugs are commonly prescribed for musculoskeletal conditions like sprains or spasms and do not cause histamine release. However, they may have side effects such as drowsiness or dizziness, so dosage and patient monitoring are crucial.
For individuals seeking non-pharmacological alternatives, physical therapy and stretching exercises can be highly effective in managing muscle tension and spasms. Techniques such as heat therapy, massage, and acupuncture have also shown promise in relieving muscle stiffness without the risk of histamine-related side effects. These methods focus on addressing the root cause of muscle tension and improving overall musculoskeletal health, making them suitable long-term solutions for many patients.
In cases where muscle relaxation is needed for chronic conditions like multiple sclerosis or cerebral palsy, botulinum toxin (Botox) injections can be considered. Botulinum toxin works by blocking nerve signals to muscles, reducing spasms and stiffness. Unlike histamine-releasing relaxants, Botox does not cause systemic histamine release, though localized reactions at the injection site may occur. This targeted approach makes it a valuable alternative for specific muscle groups.
Lastly, lifestyle modifications such as stress management, adequate hydration, and maintaining proper posture can complement or reduce the need for muscle relaxants altogether. Incorporating relaxation techniques like yoga or mindfulness can also help alleviate muscle tension naturally. By exploring these alternatives, patients and healthcare providers can tailor treatment plans to avoid histamine-releasing relaxants while effectively managing muscle-related symptoms.
Fentanyl's Link to Muscle Rigidity: What You Need to Know
You may want to see also
Frequently asked questions
Succinylcholine and mivacurium are the primary muscle relaxants associated with histamine release.
Symptoms include flushing, hypotension, bronchospasm, tachycardia, and in severe cases, anaphylaxis.
These muscle relaxants directly stimulate mast cells, leading to the release of histamine, which triggers allergic-like reactions.
No, only specific depolarizing muscle relaxants like succinylcholine and non-depolarizing agents like mivacurium are linked to histamine release.
Pretreatment with antihistamines or alternative muscle relaxants (e.g., rocuronium) can help prevent or mitigate histamine-related reactions.