The anal sphincter is a muscle that surrounds the anal canal and is divided into two parts: the internal anal sphincter and the external anal sphincter. These muscles are responsible for controlling bowel movements and facilitating defecation. The external anal sphincter is a pelvic floor muscle that is under voluntary control by the somatic nervous system, allowing it to stay contracted to maintain continence. The internal anal sphincter, on the other hand, is not under voluntary control and is responsible for providing resting pressure to the anal canal. Together, these muscles contribute to bowel continence and the control of gas and stool passage.
| Characteristics | Values |
|---|---|
| Name | Internal and External Anal Sphincter |
| Parts | Three parts: deep, superficial, and subcutaneous |
| Muscle fibres | Arranged in a spiral manner |
| Function | Controls bowel movements and facilitates defecation |
| Innervation | Extrinsic autonomic innervation via the inferior hypogastric plexus |
| Relaxation | Transient relaxation occurs during rectal distension and post-prandial rectal contraction |
| Treatment for injury | Surgical repair, biofeedback therapy, sacral nerve stimulation |
Explore related products






What You'll Learn
- The internal anal sphincter is a specialised thickened terminal portion of the inner circular layer of smooth muscle
- The external anal sphincter is under voluntary control by the somatic nervous system
- Anal sphincter injuries refer to tears or damage to the muscle surrounding the anal canal
- The external anal sphincter is located at the intersection of intricate muscle fibres and intricate anatomical spaces
- The internal anal sphincter is contracted at rest but relaxes during defecation
![]()
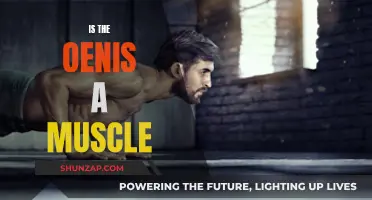
The internal anal sphincter is a specialised thickened terminal portion of the inner circular layer of smooth muscle
The anal sphincter is divided into two muscles: the internal anal sphincter and the external anal sphincter. These muscles are responsible for controlling bowel movements. The internal anal sphincter is a specialised thickened terminal portion of the inner circular layer of smooth muscle of the large intestine. It extends proximally from the pectinate line (the anorectal junction) to just proximal to the anal orifice distally. Its muscle fibres are arranged in a spiral manner, rather than a circular one.
At its distal extremity, the internal anal sphincter is in contact with the external anal sphincter, but the two muscles remain separate. The external anal sphincter is a pelvic floor muscle that is largely under voluntary control by the somatic nervous system, which allows it to remain contracted. During defecation, the muscle is voluntarily relaxed to allow the passage of faeces. The internal anal sphincter, on the other hand, is contracted in its resting state but can reflexively relax in certain contexts, most notably during defecation.
The internal anal sphincter receives extrinsic autonomic innervation via the inferior hypogastric plexus. It is innervated by sympathetic nerves derived from spinal levels L1-L2 and parasympathetic nerves derived from S2-S4. In contrast, the external anal sphincter receives somatic innervation from the inferior anal nerve, a branch of the pudendal nerve (S2-S4). The internal anal sphincter is not innervated by the pudendal nerve, which instead provides motor and sensory innervation to the external anal sphincter.
The internal anal sphincter contributes significantly to the resting pressure of the anal canal, accounting for approximately 55% of the total pressure. This pressure is crucial for bowel continence, particularly for liquids and gases. When the rectum fills beyond a certain capacity, the rectal walls distend, triggering the defecation cycle. This cycle begins with the relaxation of the internal anal sphincter, allowing a small amount of rectal contents to descend into the anal canal.
Marijuana's Surprising Benefits for Muscle Relaxation and Recovery
You may want to see also
Explore related products






![]()
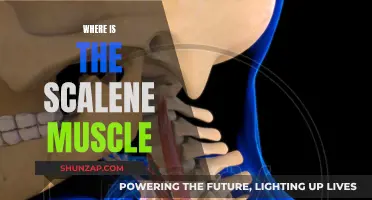
The external anal sphincter is under voluntary control by the somatic nervous system
The anal sphincter muscle is divided into two parts: the internal sphincter and the external sphincter muscle. These muscles are used to control bowel movements. The external anal sphincter is a pelvic floor muscle that facilitates defecation. It is under voluntary control by the somatic nervous system, which allows it to remain in a contracted state. This means that the muscle can be voluntarily relaxed during defecation to allow the passage of feces. The external anal sphincter is a complex muscle with a circular structure and an intricate origin and insertion pattern. It originates from the skin and fascia surrounding the anus and the anal canal.
The external anal sphincter has two separate insertions: anteriorly into the perineal body and posteriorly into the anococcygeal ligament, which stretches back to insert into the coccyx. The muscle is composed of three distinct parts or zones: the upper or deep part, the middle or superficial part, and the lower or subcutaneous part. The deep part forms a tube around the higher portion of the internal anal sphincter, while the superficial part surrounds the lower portion. The subcutaneous part surrounds the anal verge, with its most inferior fibres extending past the internal anal sphincter.
The external anal sphincter is located at the intersection of many intricate muscle fibres and is related to several anatomical structures. It forms part of the posteromedial wall of the ischioanal fossa and is connected to some muscles of the perineum. Its fibres partially blend with the puboanalis muscle, part of the pelvic diaphragm, and the superficial transverse perineal muscle. The external anal sphincter also relates to the conjoint longitudinal muscle, which lies between it and the internal anal sphincter. The conjoint longitudinal muscle sends fibres through the external anal sphincter, with inferior fibres passing through the lower subcutaneous part and outward-facing fibres through the deep part.
The external anal sphincter receives somatic innervation from the inferior anal nerve, a branch of the pudendal nerve. This innervation allows for voluntary control of the muscle. Injuries to the external anal sphincter can result in decreased control over bowel movements and accidental bowel leakage. Treatment options for such injuries include surgical repair, biofeedback therapy, and sacral nerve stimulation. Understanding the complex anatomy of the external anal sphincter is essential for effective diagnosis and treatment of any related conditions or injuries.
Speed's Impact on Muscles: Performance and Growth
You may want to see also
Explore related products





![]()
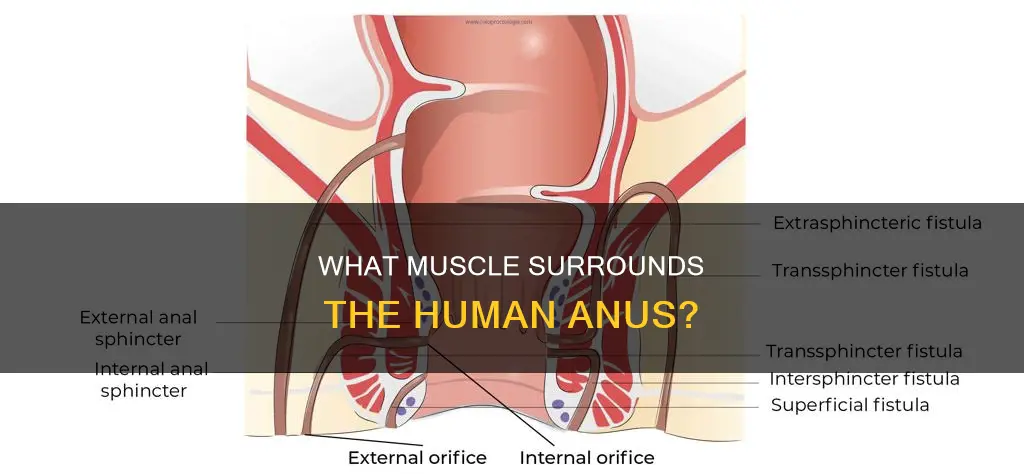
Anal sphincter injuries refer to tears or damage to the muscle surrounding the anal canal
Vaginal delivery is the most common cause of anal sphincter injury in women. About 85% of vaginal deliveries are associated with mild perineal injury, while 10% are associated with severe injuries. Anal sphincter injuries can also occur during anal or rectal surgery, or as a result of other trauma to the rectum. In some cases, anal sphincter injuries may be asymptomatic, but they usually present with fecal urgency, fecal incontinence, flatus incontinence, or dyspareunia.
The treatment for anal sphincter injuries depends on the degree of injury and the patient's presentation. Conservative management may include zinc-aluminum ointment and pelvic floor physical therapy. For more severe injuries, such as third and fourth-degree perineal tears, surgical correction may be necessary to regain anal continence. Repair techniques include end-to-end and overlap repairs. Biofeedback therapy is another treatment option that helps strengthen the muscles of the anus and pelvic floor to decrease incidents of accidental bowel leakage.
The diagnosis of anal sphincter injuries typically involves a thorough history and physical exam. The history will focus on obstetrical history, previous anorectal surgeries, other trauma to the anal canal, and current bowel habits, including the ability to control gas and stool. A digital rectal exam may also be performed by a specialized physician, such as a colon and rectal surgeon. Imaging techniques such as ultrasound, MRI, and anal manometry can also be used to evaluate the extent of the injury.
Building Lean Muscle: Strategies for Strength and Definition
You may want to see also
Explore related products






![]()
The external anal sphincter is located at the intersection of intricate muscle fibres and intricate anatomical spaces
The external anal sphincter is a complex muscle with a unique origin and insertion pattern. It is a pelvic floor muscle that plays a crucial role in facilitating defecation. The muscle is typically described as originating from the skin and fascia surrounding the anus and the anal canal. It has two distinct insertions: anteriorly into the perineal body and posteriorly into the anococcygeal ligament, which extends posteriorly to insert into the coccyx.
The external anal sphincter is closely associated with the conjoint longitudinal muscle, which lies between the external and internal anal sphincters. The conjoint longitudinal muscle sends fibres through the external anal sphincter, with inferior fibres passing through the lower subcutaneous part and outward-facing fibres traversing the deep part. The space between the external anal sphincter and the conjoint longitudinal muscle is known as the intersphincteric space, which houses anal glands.
The intricate anatomy of the external anal sphincter extends beyond its muscular connections. It is contained within the anal triangle, along with the anococcygeal ligament and the inferior anal nerve. The external anal sphincter forms a part of the posteromedial wall of the ischioanal fossa. Additionally, its fibres blend with other muscles, including the puboanalis muscle, a component of the pelvic diaphragm, and the superficial transverse perineal muscle.
The external anal sphincter is under voluntary control by the somatic nervous system, allowing it to remain contracted to maintain continence. During defecation, it is voluntarily relaxed to permit the passage of feces. This complex interplay between muscular anatomy and nervous system control ensures the proper functioning of the external anal sphincter, contributing to bowel continence and facilitating defecation when needed.
Understanding Muscle Function: The Basics of How They Work
You may want to see also
Explore related products

![]()
The internal anal sphincter is contracted at rest but relaxes during defecation
The internal anal sphincter (IAS) is a ring of smooth muscle that surrounds the anal canal. It is about 5mm thick and is formed by an aggregation of the smooth circular muscle fibres of the rectum. The IAS is normally in a state of continuous maximal contraction to prevent the leakage of faeces or gases. This contraction is stimulated and maintained by sympathetic stimulation, which is mediated by alpha-2 adrenergic receptors. The IAS is the thickened terminal portion of the inner circular layer of the large intestine. It extends from the pectinate line (anorectal junction) proximally to just proximal to the anal orifice distally.
The external anal sphincter is a pelvic floor muscle that facilitates defecation. It is controlled by somatic nerve supply from the inferior anal branch of the pudendal nerve, which allows conscious control of defecation. The external sphincter is voluntarily relaxed during defecation to allow the passage of faeces. The internal and external anal sphincters work together to control the expulsion of faeces. The external sphincter is related to the conjoint longitudinal muscle, which sends fibres through the external anal sphincter. The external anal sphincter is located at the intersection of many intricate muscle fibres and is connected to several anatomical structures, including the anal triangle and the ischioanal fossa.
The internal anal sphincter is an important component of the digestive system, working in conjunction with the external anal sphincter to regulate the passage of faeces. Its ability to contract at rest and relax during defecation is essential for maintaining continence and facilitating the expulsion of waste.
Activating Your Soleus Muscle: Simple and Effective Techniques
You may want to see also
Frequently asked questions
The anal sphincter is divided into two muscles: the internal anal sphincter and the external anal sphincter. These muscles control bowel movements.
The internal anal sphincter is a specialised thickened terminal portion of the inner circular layer of smooth muscle of the large intestine. It is contracted in its resting state but relaxes during defecation.
The external anal sphincter is a pelvic floor muscle that is under voluntary control by the somatic nervous system. It stays contracted to maintain continence and is relaxed during defecation to allow the passage of faeces.
An anal sphincter injury refers to a tear or damage to the internal or external sphincter muscle that surrounds the anal canal. This can result in decreased control over bowel movements and accidental bowel leakage.