Muscle relaxers and neuromuscular blocking drugs (NMBDs) are often confused due to their similar-sounding names, but they serve distinct purposes and function differently in the body. Muscle relaxers, such as cyclobenzaprine or baclofen, are typically used to alleviate muscle spasms and pain by acting on the central nervous system, helping to reduce tension and improve mobility. In contrast, NMBDs, like succinylcholine or rocuronium, are powerful medications used in anesthesia to induce temporary paralysis by blocking the transmission of signals between nerves and muscles, ensuring complete relaxation during surgical procedures. While both types of drugs affect muscle function, their mechanisms, applications, and risks differ significantly, making them entirely separate classes of medications.
| Characteristics | Values |
|---|---|
| Definition | Muscle relaxers and Neuromuscular Blocking Drugs (NMBDs) are distinct classes of drugs. Muscle relaxers act centrally to reduce muscle tone, while NMBDs act peripherally to block neuromuscular transmission. |
| Mechanism of Action | Muscle relaxers: Act on the central nervous system (CNS) to reduce muscle spasms. NMBDs: Block acetylcholine receptors at the neuromuscular junction, causing paralysis. |
| Primary Use | Muscle relaxers: Treat muscle spasms, pain, and stiffness. NMBDs: Facilitate endotracheal intubation and muscle relaxation during surgery. |
| Administration | Muscle relaxers: Oral, injectable, or topical. NMBDs: Intravenous or intramuscular (primarily IV in clinical settings). |
| Duration of Action | Muscle relaxers: Short to moderate duration (hours). NMBDs: Short-acting (minutes to hours) or long-acting (hours). |
| Examples | Muscle relaxers: Cyclobenzaprine, Baclofen, Tizanidine. NMBDs: Succinylcholine, Rocuronium, Vecuronium. |
| Side Effects | Muscle relaxers: Drowsiness, dizziness, dry mouth. NMBDs: Muscle weakness, prolonged paralysis (if not reversed), respiratory depression. |
| Reversibility | Muscle relaxers: Effects wear off naturally. NMBDs: Effects can be reversed with anticholinesterase drugs (e.g., neostigmine). |
| Clinical Setting | Muscle relaxers: Outpatient use for musculoskeletal conditions. NMBDs: Primarily used in anesthesia and critical care. |
| Dependency Risk | Muscle relaxers: Potential for dependence with long-term use. NMBDs: No risk of dependence; used only in controlled settings. |
| Monitoring Required | Muscle relaxers: Minimal monitoring. NMBDs: Continuous monitoring of respiratory function and neuromuscular blockade. |
Explore related products






What You'll Learn
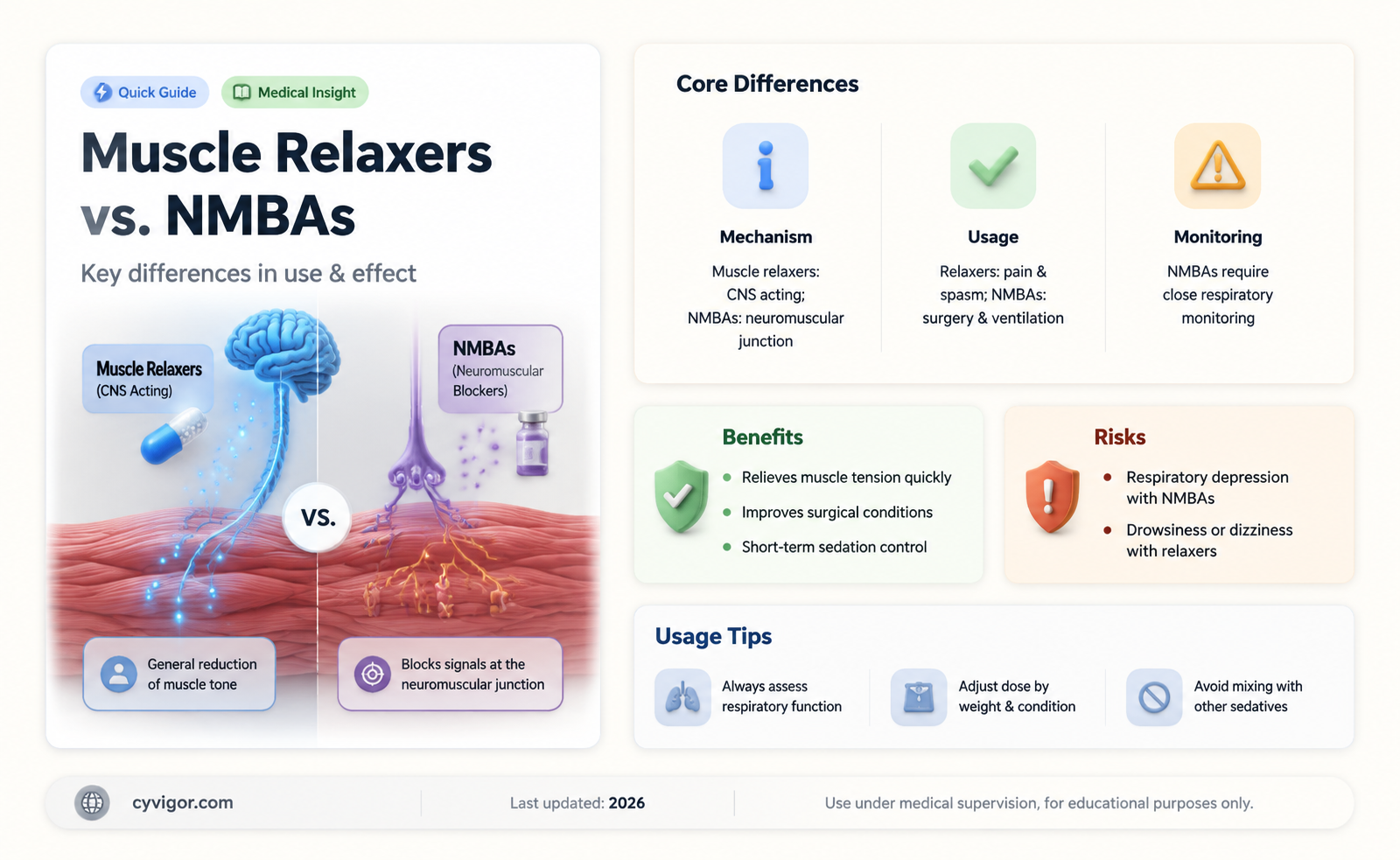
- Definition Differences: Muscle relaxers reduce muscle spasms; NMBAs (Neuromuscular Blocking Agents) paralyze muscles for procedures
- Mechanism of Action: Relaxers act on CNS; NMBAs block neuromuscular junction signals
- Medical Uses: Relaxers for pain relief; NMBAs for surgery or ventilation
- Side Effects: Relaxers cause drowsiness; NMBAs risk respiratory depression
- Administration: Relaxers oral/IV; NMBAs typically IV in controlled settings
![]()
Definition Differences: Muscle relaxers reduce muscle spasms; NMBAs (Neuromuscular Blocking Agents) paralyze muscles for procedures
Muscle relaxers and Neuromuscular Blocking Agents (NMBAs) are often conflated, yet their mechanisms and purposes diverge sharply. Muscle relaxers, such as cyclobenzaprine or tizanidine, target the central nervous system to alleviate muscle spasms caused by conditions like back pain or multiple sclerosis. They work by reducing nerve impulses, allowing muscles to relax without directly paralyzing them. In contrast, NMBAs like succinylcholine or rocuronium act peripherally at the neuromuscular junction, blocking nerve signals to muscles entirely, resulting in temporary paralysis. This distinction is critical: muscle relaxers are prescribed for chronic or acute spasms, often in oral doses (e.g., 5–10 mg of cyclobenzaprine up to three times daily), while NMBAs are administered intravenously in controlled medical settings, such as during surgery or intubation, to ensure complete muscle immobility.
Consider the practical implications of these differences. A patient with a strained back might take a muscle relaxer to ease spasms and improve mobility, but they remain conscious and able to move voluntarily. Conversely, NMBAs render patients completely paralyzed, necessitating mechanical ventilation and continuous monitoring by anesthesiologists. For instance, succinylcholine, a depolarizing NMBA, is used for rapid sequence intubation but has a short duration (5–10 minutes), whereas non-depolarizing agents like rocuronium provide longer paralysis (30–90 minutes) and are reversed with drugs like neostigmine. Misusing NMBAs outside a clinical setting could lead to respiratory arrest, underscoring their specialized role.
The age and condition of the patient further highlight these differences. Muscle relaxers are commonly prescribed for adults with musculoskeletal injuries or neurological disorders, though caution is advised in elderly patients due to increased sedation and fall risks. NMBAs, however, are reserved for procedural use across all age groups, from neonates to the elderly, but require precise dosing based on factors like renal function and comorbidities. For example, a pediatric patient undergoing spinal surgery might receive a lower dose of rocuronium (0.6 mg/kg) compared to an adult (0.6–1.2 mg/kg), with real-time monitoring of muscle response via a peripheral nerve stimulator.
From a clinical perspective, the choice between a muscle relaxer and an NMBA hinges on the desired outcome. Muscle relaxers aim to relieve pain and improve function, often as part of a broader treatment plan including physical therapy. NMBAs, however, are tools of acute intervention, enabling procedures like tracheal intubation or facilitating surgical access by eliminating muscle tone. While both classes affect muscle activity, their applications are mutually exclusive: one treats spasms, the other induces paralysis. Understanding this distinction ensures appropriate use, minimizes risks, and optimizes patient outcomes.
Is Midol a Muscle Relaxer? Understanding Its Uses and Effects
You may want to see also
Explore related products






![]()
Mechanism of Action: Relaxers act on CNS; NMBAs block neuromuscular junction signals
Muscle relaxers and neuromuscular blocking agents (NMBAs) are often confused due to their shared goal of reducing muscle activity, but their mechanisms of action are fundamentally different. Muscle relaxers, such as cyclobenzaprine and tizanidine, primarily act on the central nervous system (CNS). They depress neuronal activity in the brain and spinal cord, reducing the transmission of nerve signals that lead to muscle contraction. This systemic approach makes them effective for conditions like muscle spasms or pain but also increases the risk of side effects such as drowsiness, dizziness, and impaired coordination. Dosages typically range from 5 to 30 mg, depending on the specific drug and patient needs, and they are often prescribed for short-term use due to their potential for dependence.
In contrast, NMBAs, such as succinylcholine and rocuronium, operate at the neuromuscular junction (NMJ), the site where nerve cells communicate with muscle fibers. These agents block the receptors for acetylcholine, the neurotransmitter responsible for initiating muscle contraction. By preventing acetylcholine from binding to its receptors, NMBAs induce paralysis, making them essential in surgical settings for procedures requiring complete muscle relaxation. Unlike muscle relaxers, NMBAs do not cross the blood-brain barrier and thus do not affect the CNS. However, their use requires careful monitoring, as they can cause respiratory depression and other complications if not administered with precision. Dosages are highly individualized, often starting at 0.6 mg/kg for succinylcholine, and are typically administered intravenously by trained medical professionals.
The distinct mechanisms of these two classes of drugs highlight their appropriate applications. Muscle relaxers are best suited for outpatient management of musculoskeletal conditions, where mild to moderate sedation is acceptable. For instance, a patient with acute lower back pain might benefit from a 10 mg dose of cyclobenzaprine at bedtime to alleviate spasms and improve sleep. On the other hand, NMBAs are reserved for controlled environments like operating rooms, where temporary paralysis is necessary for procedures such as intubation or complex surgeries. Their rapid onset and short duration of action, particularly with succinylcholine, make them ideal for such scenarios, but they are never used without concurrent ventilation support.
Understanding these differences is crucial for both healthcare providers and patients. Misuse or confusion between the two can lead to serious adverse effects. For example, administering an NMBA outside of a surgical setting without respiratory support could be life-threatening. Conversely, over-reliance on muscle relaxers for chronic conditions may lead to tolerance or addiction. Practical tips include always verifying the intended use of the medication, ensuring proper monitoring during administration, and educating patients about potential side effects. For instance, patients on muscle relaxers should avoid driving or operating heavy machinery until they know how the drug affects them.
In summary, while both muscle relaxers and NMBAs reduce muscle activity, their mechanisms of action—CNS depression versus NMJ blockade—dictate their uses, risks, and administration protocols. Muscle relaxers are systemic agents for outpatient pain management, whereas NMBAs are specialized tools for surgical paralysis. Recognizing these distinctions ensures safer and more effective treatment, whether in a clinic or an operating room. Always consult a healthcare professional for personalized guidance on dosage, duration, and precautions.
Muscle Relaxers and Viagra: Potential Interactions and Effects Explained
You may want to see also
Explore related products






![]()
Medical Uses: Relaxers for pain relief; NMBAs for surgery or ventilation
Muscle relaxers and neuromuscular blocking agents (NMBAs) serve distinct medical purposes, despite both targeting muscle function. Muscle relaxers, such as cyclobenzaprine or tizanidine, are commonly prescribed for musculoskeletal pain relief. They work by reducing muscle spasms and tension, often alleviating conditions like lower back pain or neck stiffness. These medications are typically taken orally, with dosages ranging from 5 to 30 mg daily, depending on the specific drug and patient needs. For instance, cyclobenzaprine is often started at 5 mg three times a day, while tizanidine may be prescribed at 2–4 mg every 6–8 hours. It’s crucial to avoid alcohol and sedatives when using these relaxers, as they can enhance drowsiness and impair coordination.
In contrast, NMBAs are used in critical medical scenarios, primarily during surgery or mechanical ventilation. These agents, such as succinylcholine or rocuronium, induce temporary paralysis by blocking neuromuscular transmission, ensuring complete muscle relaxation. This is essential for procedures like intubation or complex surgeries where muscle movement could interfere. NMBAs are administered intravenously, with dosages tailored to the patient’s weight and the procedure’s requirements. For example, succinylcholine is often given as a rapid bolus of 1–2 mg/kg, while rocuronium may be dosed at 0.6–1.2 mg/kg. Unlike muscle relaxers, NMBAs require continuous monitoring and reversal agents like sugammadex to restore muscle function post-procedure.
The contexts in which these medications are used highlight their differences. Muscle relaxers are outpatient treatments, often prescribed for short-term pain management in adults. They are not recommended for long-term use due to risks like dependence or tolerance. Conversely, NMBAs are exclusively used in hospital settings, typically in operating rooms or intensive care units, under the supervision of anesthesiologists or critical care specialists. Their use is strictly controlled, as improper administration can lead to respiratory depression or prolonged paralysis.
Practical considerations further distinguish these two classes. Muscle relaxers can be taken at home, but patients should avoid driving or operating machinery due to potential side effects like dizziness. NMBAs, however, require a controlled environment with immediate access to ventilatory support and reversal agents. For instance, a patient receiving rocuronium for surgery must be intubated and ventilated until the drug’s effects wear off or are reversed. This underscores the specialized nature of NMBAs compared to the more accessible use of muscle relaxers.
In summary, while both muscle relaxers and NMBAs modulate muscle activity, their applications, mechanisms, and settings of use are fundamentally different. Muscle relaxers offer pain relief for musculoskeletal conditions, whereas NMBAs facilitate critical medical procedures by inducing temporary paralysis. Understanding these distinctions ensures appropriate use and highlights the importance of tailored medical interventions for specific clinical needs.
Cortisone and Muscle Relaxation: Unraveling the Truth Behind the Myth
You may want to see also
![]()
Side Effects: Relaxers cause drowsiness; NMBAs risk respiratory depression
Muscle relaxers and neuromuscular blocking agents (NMBAs) are distinct classes of drugs with different mechanisms and side effects, yet both carry significant risks that demand careful consideration. While muscle relaxers, such as cyclobenzaprine or tizanidine, primarily target the central nervous system to alleviate muscle spasms, they often induce drowsiness as a common side effect. This sedation can impair daily activities, such as driving or operating machinery, and is more pronounced in elderly patients or those taking higher doses (e.g., cyclobenzaprine 10 mg twice daily). In contrast, NMBAs like succinylcholine or rocuronium act peripherally at the neuromuscular junction to induce paralysis, posing a far more critical risk: respiratory depression. This life-threatening complication requires immediate intervention, including mechanical ventilation, making NMBAs suitable only for controlled settings like surgery or intensive care.
The drowsiness caused by muscle relaxers, though less severe than NMBA-induced respiratory depression, is not without consequence. Patients prescribed these medications should be advised to avoid alcohol and other sedatives, as combining these substances can exacerbate drowsiness and increase fall risks, particularly in adults over 65. For instance, tizanidine’s sedative effects are dose-dependent, with 4 mg doses already causing noticeable drowsiness in some individuals. To mitigate this, starting with the lowest effective dose (e.g., 2 mg) and gradually titrating upward can help balance efficacy and tolerability. Conversely, NMBAs’ respiratory risks are inherent to their mechanism, necessitating constant monitoring of vital signs and readiness to administer reversal agents like sugammadex or neostigmine in emergencies.
A comparative analysis highlights the divergent safety profiles of these drugs. Muscle relaxers’ side effects are manageable with patient education and dose adjustments, making them suitable for outpatient use in conditions like acute back pain. NMBAs, however, are reserved for specific clinical scenarios where paralysis is necessary, such as endotracheal intubation or surgical procedures requiring muscle relaxation. Their use is strictly contraindicated in patients with respiratory compromise or neuromuscular disorders, as these conditions heighten the risk of prolonged paralysis or respiratory failure. For example, succinylcholine’s rapid onset (30–60 seconds) and short duration (5–10 minutes) make it ideal for brief procedures, but its potential to trigger hyperkalemia in susceptible populations underscores the need for meticulous patient selection.
Practitioners must differentiate between these drugs to avoid catastrophic errors. Confusing a muscle relaxer for an NMBA, or vice versa, could lead to inappropriate dosing or administration, with dire consequences. For instance, administering rocuronium (an NMBA) instead of a muscle relaxer like baclofen would result in immediate paralysis and respiratory arrest in an outpatient setting. Conversely, using a muscle relaxer in a surgical context where complete paralysis is required would render the procedure unfeasible. Clear labeling, double-checking drug names, and interdisciplinary communication are essential to prevent such mix-ups.
In summary, while both muscle relaxers and NMBAs carry risks, their side effects differ markedly in severity and management. Drowsiness from muscle relaxers can be minimized through cautious prescribing and patient counseling, whereas NMBAs’ respiratory depression demands a controlled environment and emergency preparedness. Understanding these distinctions is critical for safe and effective use, ensuring that the right drug is chosen for the right patient in the right context.
Can Muscle Relaxers Cause Stomach Upset? Understanding Side Effects
You may want to see also
![]()
Administration: Relaxers oral/IV; NMBAs typically IV in controlled settings
Muscle relaxers and neuromuscular blocking agents (NMBAs) differ significantly in their administration routes, reflecting their distinct purposes and safety profiles. Muscle relaxers, such as cyclobenzaprine or tizanidine, are commonly prescribed orally in tablet or capsule form, with dosages ranging from 5 to 30 mg daily, depending on the medication and patient needs. These oral formulations allow for convenient at-home use, often for conditions like muscle spasms or chronic pain. In contrast, NMBAs, such as succinylcholine or rocuronium, are almost exclusively administered intravenously (IV) in controlled medical settings like operating rooms or intensive care units. This IV route ensures rapid onset and precise titration, critical for procedures requiring complete muscle paralysis, such as intubation or surgery.
The choice of administration route is tied to the drugs' mechanisms and risks. Oral muscle relaxers act centrally on the nervous system, reducing muscle tone without causing paralysis, making them safe for outpatient use. IV administration of these drugs is rare and typically reserved for specific cases, such as severe spasticity, where a faster effect is needed. NMBAs, however, act peripherally at the neuromuscular junction, inducing temporary paralysis, which demands immediate medical oversight. Their IV delivery is essential to manage potential complications like respiratory depression, requiring mechanical ventilation until the drug's effects wear off.
Practical considerations further highlight the differences. Oral muscle relaxers often come with instructions to take with food or at bedtime to minimize side effects like drowsiness. Patients are advised to avoid alcohol and activities requiring alertness until they know how the drug affects them. For NMBAs, administration is a tightly controlled process involving trained anesthesiologists or critical care teams. Dosages are tailored to patient factors like weight, age, and renal function, with monitoring tools like nerve stimulators used to assess muscle response and adjust dosing in real time.
In summary, the administration of muscle relaxers and NMBAs underscores their divergent roles in healthcare. Oral or occasional IV use of muscle relaxers supports outpatient management of musculoskeletal conditions, while the exclusive IV administration of NMBAs in controlled environments ensures safety during high-stakes medical procedures. Understanding these differences is crucial for both healthcare providers and patients to optimize therapeutic outcomes and minimize risks.
Effective Techniques to Relax Your Intercostal Muscles and Ease Tension
You may want to see also
Frequently asked questions
No, muscle relaxers and NMBDs are not the same. Muscle relaxers (e.g., cyclobenzaprine, baclofen) are used to relieve muscle spasms and pain by acting on the central nervous system, while NMBDs (e.g., succinylcholine, vecuronium) are used in anesthesia to cause temporary paralysis by blocking nerve signals to muscles.
No, muscle relaxers do not cause paralysis. They reduce muscle tension and spasms but do not completely block nerve signals to muscles, unlike NMBDs, which induce temporary paralysis for medical procedures.
No, they are used for different purposes. Muscle relaxers are prescribed for conditions like muscle spasms, back pain, or injuries, while NMBDs are used in surgical settings to facilitate intubation or prevent muscle movement during procedures.
No, their side effects differ. Muscle relaxers may cause drowsiness, dizziness, or dry mouth, while NMBDs can lead to respiratory paralysis, requiring mechanical ventilation, and may cause allergic reactions or prolonged paralysis in rare cases.
No, muscle relaxers cannot replace NMBDs in surgery. NMBDs are specifically designed to induce complete muscle paralysis for procedures, whereas muscle relaxers do not provide the same level of muscle control or paralysis needed for surgical interventions.