The abduction of the arm, which involves moving the arm away from the body in the frontal plane, is primarily facilitated by the deltoid muscle, specifically its middle fibers. However, the supraspinatus muscle, one of the rotator cuff muscles, also plays a crucial role in initiating this movement by stabilizing the shoulder joint and assisting in the initial phase of abduction. Understanding which muscles are responsible for this action is essential for comprehending shoulder anatomy, function, and potential injuries related to arm movement.
| Characteristics | Values |
|---|---|
| Muscle Name | Deltoid |
| Primary Action | Arm abduction (moving the arm away from the body in the frontal plane) |
| Origin | Clavicle (anterior fibers), acromion (middle fibers), spine of the scapula (posterior fibers) |
| Insertion | Deltoid tuberosity of the humerus |
| Nerve Supply | Axillary nerve (C5-C6) |
| Blood Supply | Posterior circumflex humeral artery, deltoid branch of the thoracoacromial artery |
| Fiber Direction | Multipennate (fibers converge at an angle to the tendon) |
| Antagonist Muscle | Pectoralis major, latissimus dorsi (during adduction) |
| Additional Actions | Shoulder flexion (anterior fibers), shoulder extension (posterior fibers), lateral rotation (posterior fibers) |
| Innervation | Axillary nerve (C5-C6) |
| Common Injuries | Strains, tendonitis, tears (especially in athletes or with repetitive overhead activities) |
| Function in Daily Life | Lifting objects sideways, reaching overhead, stabilizing the shoulder during movement |
Explore related products






What You'll Learn
- Supraspinatus Role: Supraspinatus initiates arm abduction, working with deltoid for shoulder movement
- Deltoid Function: Deltoid muscle is primary abductor, lifting arm away from body
- Rotator Cuff: Supraspinatus, part of rotator cuff, stabilizes during abduction
- Nerve Supply: Supraspinatus innervated by suprascapular nerve; deltoid by axillary nerve
- Abduction Range: Full abduction is 0° to 180°, involving multiple muscles
![]()
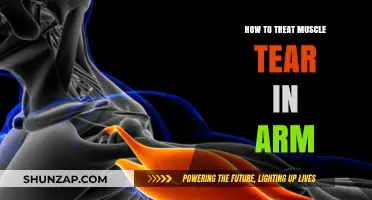
Supraspinatus Role: Supraspinatus initiates arm abduction, working with deltoid for shoulder movement
The supraspinatus muscle, though small, plays a pivotal role in the complex mechanics of arm abduction. Nestled within the supraspinous fossa of the scapula, it acts as the initiator of this movement, firing first to lift the arm away from the body. This initial action is crucial, as it stabilizes the humeral head within the glenoid fossa, creating a stable foundation for the deltoid muscle to take over and complete the abduction process. Without the supraspinatus, the deltoid would struggle to efficiently lift the arm, leading to compensatory movements that could strain other shoulder structures.
Consider the practical implications of this muscle’s function. For instance, during exercises like lateral raises, the supraspinatus engages first, subtly lifting the arm before the deltoid fully activates. This sequential activation is why individuals with supraspinatus injuries often experience weakness or pain during the initial phase of arm abduction, even if the deltoid remains strong. Physical therapists often emphasize isolated supraspinatus strengthening exercises, such as external rotation with a resistance band, to restore this critical initiation phase. For adults over 40, who are more prone to supraspinatus tears, incorporating these exercises into a routine can prevent dysfunction and maintain shoulder health.
A comparative analysis highlights the supraspinatus’s unique contribution. While the deltoid is the prime mover for abduction, the supraspinatus acts as a stabilizer and initiator, akin to a conductor starting an orchestra. This distinction becomes evident in rehabilitation settings, where patients with supraspinatus injuries often exhibit a "lag sign"—a delay in arm elevation during abduction. In contrast, deltoid injuries typically result in a complete inability to lift the arm beyond a certain point. Understanding this difference is essential for accurate diagnosis and targeted treatment, ensuring that therapy addresses the root cause of the impairment.
From a persuasive standpoint, prioritizing supraspinatus health is non-negotiable for anyone engaged in repetitive overhead activities, such as athletes or manual laborers. Overuse or improper mechanics can lead to impingement and eventual tearing of this muscle, a condition commonly referred to as "swimmer’s shoulder." To mitigate this risk, incorporate scapular stabilization exercises, such as wall slides or prone Y-T-I raises, into your routine. These movements reinforce the supraspinatus’s role in maintaining proper shoulder alignment, reducing the likelihood of injury. For those already experiencing symptoms, early intervention—including rest, ice, and physical therapy—can prevent chronic issues and the need for surgical repair.
Finally, a descriptive exploration of the supraspinatus’s anatomy underscores its functional importance. Originating from the supraspinous fossa, it inserts onto the greater tubercle of the humerus via a thin, vulnerable tendon. This tendon’s proximity to the acromion makes it susceptible to impingement, particularly in individuals with bony abnormalities or poor posture. Visualizing this structure during movement—such as the subtle lift of the arm during the first 15 degrees of abduction—reinforces its indispensable role. By appreciating the supraspinatus’s anatomy and function, individuals can better protect this muscle, ensuring smooth and pain-free shoulder movement throughout life.
Understanding the Key Muscle Driving Arm Abduction: A Comprehensive Guide
You may want to see also
Explore related products






![]()
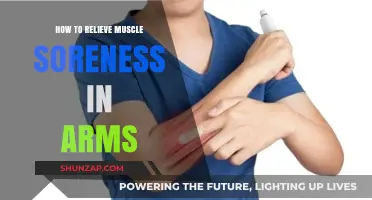
Deltoid Function: Deltoid muscle is primary abductor, lifting arm away from body
The deltoid muscle, a triangular powerhouse nestled atop the shoulder, serves as the primary architect of arm abduction. This fundamental movement, lifting the arm away from the body, is a cornerstone of daily activities—from reaching for a shelf to waving hello. Understanding the deltoid’s role in abduction not only enhances anatomical knowledge but also optimizes strength training and injury prevention.
Anatomically, the deltoid comprises three distinct heads: anterior, lateral, and posterior. While all contribute to shoulder movement, the lateral head is the star player in abduction. When activated, it initiates the outward lifting motion, working in harmony with the supraspinatus muscle, which stabilizes the shoulder joint. This synergy ensures smooth, controlled movement, particularly in the initial 15 degrees of abduction, where the supraspinatus takes the lead before the deltoid fully engages.
To effectively target the deltoid during abduction exercises, consider lateral raises as a staple. Stand with feet shoulder-width apart, hold dumbbells at your sides, and lift your arms outward until they reach shoulder height. Maintain a slight bend in the elbows and avoid leaning backward. For optimal results, perform 3 sets of 12–15 repetitions, adjusting weight to challenge the muscle without compromising form. Beginners should start with lighter weights to build endurance, while advanced lifters can incorporate resistance bands for added intensity.
A common pitfall in abduction exercises is over-reliance on momentum, which diminishes the deltoid’s engagement. To maximize effectiveness, focus on slow, deliberate movements, emphasizing the mind-muscle connection. Additionally, ensure proper warm-up to prevent strains, as the shoulder joint is highly susceptible to injury. Rotator cuff stretches and light arm circles can prepare the deltoid and surrounding structures for activity.
Incorporating deltoid-focused abduction exercises into your routine not only strengthens the shoulder but also enhances functional mobility. Whether you’re an athlete, fitness enthusiast, or simply seeking to improve daily movement, mastering this muscle’s role in abduction is a game-changer. By combining correct technique, progressive resistance, and mindful practice, you can unlock the full potential of the deltoid, ensuring both strength and stability in every lift.
Master Arm Wrestling: Key Muscles to Train for Strength & Power
You may want to see also
Explore related products






![]()
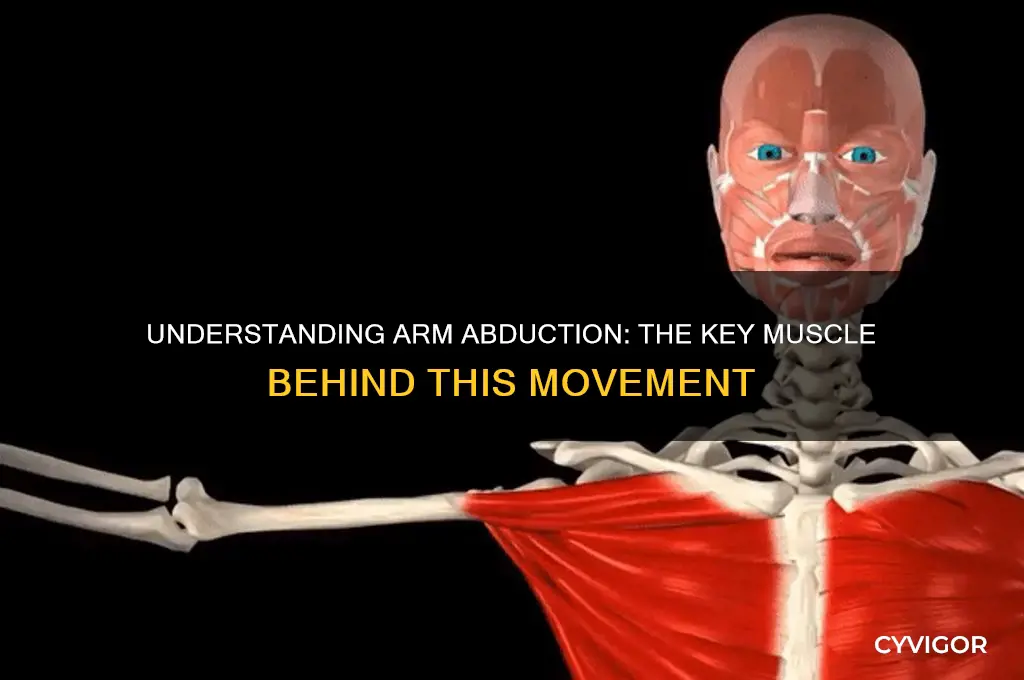
Rotator Cuff: Supraspinatus, part of rotator cuff, stabilizes during abduction
The supraspinatus muscle, a key player in the rotator cuff group, is often overlooked in discussions about arm abduction, yet its role is indispensable. While the deltoid muscle is primarily responsible for lifting the arm away from the body, the supraspinatus ensures this movement occurs smoothly and without instability. This small but mighty muscle initiates abduction by lifting the arm the first 15 degrees, after which the deltoid takes over. Without the supraspinatus, even the simplest tasks like reaching for a shelf or waving goodbye would be compromised, leading to discomfort or injury.
Consider the mechanics: the supraspinatus originates in the supraspinous fossa of the scapula and inserts on the greater tubercle of the humerus. Its primary function is to stabilize the humeral head in the glenoid fossa during abduction, preventing it from migrating upward. This stabilization is crucial because the shoulder joint, while highly mobile, is inherently unstable due to its shallow socket. For instance, during a lateral raise, the supraspinatus contracts isometrically to keep the humeral head centered, allowing the deltoid to act efficiently. Weakness or injury to this muscle often results in impingement syndrome, a common cause of shoulder pain in adults over 40.
To strengthen the supraspinatus and prevent dysfunction, targeted exercises are essential. One effective movement is the empty can exercise, named for the position of the arm resembling a discarded can. Stand with your arms at your sides, then raise them to 45 degrees in front of your body, thumbs pointing downward. Slowly lift your arms until they’re parallel to the floor, ensuring the movement is controlled. Perform 3 sets of 12–15 repetitions, 2–3 times per week. Avoid overexertion, as the supraspinatus is prone to strain, especially in individuals who engage in repetitive overhead activities like swimming or tennis.
Comparatively, while the deltoid is the powerhouse of arm abduction, the supraspinatus is the unsung hero that ensures precision and safety. Think of the deltoid as the engine of a car and the supraspinatus as the suspension system—both are vital, but one stabilizes while the other propels. This analogy underscores the importance of maintaining balance between strength and stability in shoulder function. For athletes or active individuals, incorporating supraspinatus-specific exercises into a routine can reduce the risk of injury by 30%, according to a study published in the *Journal of Orthopaedic & Sports Physical Therapy*.
In conclusion, the supraspinatus may not be the primary abductor of the arm, but its role in stabilizing the shoulder during abduction is irreplaceable. By understanding its function and incorporating targeted exercises, individuals can enhance shoulder health and prevent common injuries. Whether you’re a weekend warrior or a desk worker, prioritizing the supraspinatus ensures your arms remain strong, stable, and pain-free.
Arm Wrestling Muscles: Key Strengths for Dominating the Table
You may want to see also
Explore related products






![]()
Nerve Supply: Supraspinatus innervated by suprascapular nerve; deltoid by axillary nerve
The supraspinatus and deltoid muscles are key players in arm abduction, but their functions are distinct, and so are their nerve supplies. Understanding this neural anatomy is crucial for diagnosing and treating injuries or conditions affecting shoulder mobility. The supraspinatus, a rotator cuff muscle, initiates abduction by lifting the arm from the resting position, while the deltoid takes over to continue the movement. This division of labor is mirrored in their innervation: the supraspinatus is supplied by the suprascapular nerve, and the deltoid by the axillary nerve.
From an analytical perspective, the suprascapular nerve originates from the upper trunk of the brachial plexus (C5-C6) and travels beneath the trapezius to innervate the supraspinatus. Damage to this nerve, often due to trauma or compression, can result in supraspinatus weakness, manifesting as difficulty initiating arm abduction. For instance, athletes or laborers who repeatedly perform overhead activities may experience suprascapular nerve entrapment, leading to a condition known as suprascapular neuropathy. Early diagnosis through nerve conduction studies and targeted rehabilitation can prevent long-term dysfunction.
In contrast, the axillary nerve, arising from the posterior cord of the brachial plexus (C5-C6), innervates the deltoid and provides sensory supply to a small area of the shoulder. Axillary nerve injuries are commonly associated with shoulder dislocations or fractures of the humeral neck. A patient with axillary nerve damage may present with a characteristic "quadrangular space syndrome," where deltoid weakness and atrophy are prominent, significantly impairing the ability to abduct the arm beyond 15 degrees. Surgical intervention, such as nerve decompression or repair, may be necessary in severe cases, followed by physical therapy to restore strength and range of motion.
Practically, clinicians and therapists must differentiate between suprascapular and axillary nerve injuries to tailor treatment effectively. For suprascapular nerve issues, conservative management includes avoiding aggravating activities, anti-inflammatory medications, and targeted exercises to strengthen the supraspinatus. In axillary nerve injuries, early immobilization of the shoulder followed by gradual mobilization is critical to prevent adhesive capsulitis. Patients should be educated on proper body mechanics and ergonomic adjustments to reduce recurrence risk, especially in occupational settings.
In conclusion, the nerve supply to the supraspinatus and deltoid is not just a detail in anatomy but a cornerstone for clinical decision-making. Recognizing the unique roles of the suprascapular and axillary nerves allows for precise diagnosis and treatment, ensuring optimal recovery of arm abduction function. Whether through conservative measures or surgical intervention, addressing nerve-specific pathologies is essential for restoring shoulder health and preventing chronic disability.
Explore related products





![]()
Abduction Range: Full abduction is 0° to 180°, involving multiple muscles
The human arm's abduction range is a remarkable feat of anatomical engineering, spanning a full 180 degrees from the body's midline. This movement is not the work of a single muscle but rather a coordinated effort involving multiple muscular groups, each contributing to the seamless execution of this action. At the forefront of this process is the deltoid muscle, particularly its middle fibers, which are primarily responsible for the initial abduction from 0° to 90°. However, to achieve the full 180° range, the supraspinatus, trapezius, and serratus anterior muscles play crucial supporting roles, especially in stabilizing the scapula and allowing for the arm to move freely beyond the shoulder's lateral plane.
To maximize abduction range and strength, targeted exercises can be incorporated into a fitness regimen. For instance, lateral raises primarily engage the deltoid, enhancing its capacity to lift the arm away from the body. This exercise can be performed with dumbbells, resistance bands, or even body weight, depending on the individual's fitness level. It’s essential to maintain proper form, keeping the elbow slightly bent and the movement controlled to avoid strain. For those seeking greater challenge, variations such as bent-over lateral raises can be introduced, which also engage the trapezius and rhomboids, further supporting scapular stability.
A comparative analysis of abduction across different age groups reveals interesting trends. Younger individuals, particularly those in their 20s and 30s, typically exhibit a fuller range of motion due to greater muscle flexibility and joint health. However, as individuals age, factors such as muscle atrophy, joint stiffness, and decreased physical activity can limit abduction range. For older adults, gentle stretching exercises and low-impact strength training can help maintain mobility. Incorporating activities like yoga or tai chi can also improve flexibility and balance, reducing the risk of injury during abduction movements.
From a practical standpoint, understanding the mechanics of arm abduction is vital for injury prevention and rehabilitation. Overuse or improper technique in activities like weightlifting or sports can lead to strains or tears in the deltoid or rotator cuff muscles. Physical therapists often emphasize the importance of progressive training, starting with lighter weights and gradually increasing resistance to build strength without compromising joint integrity. Additionally, incorporating rest days and proper warm-up routines can significantly reduce the likelihood of injury, ensuring that the muscles involved in abduction remain healthy and functional.
In conclusion, the full abduction range of the arm from 0° to 180° is a complex process that relies on the interplay of multiple muscles. By understanding the roles of these muscles and implementing targeted exercises, individuals can enhance their abduction capabilities while minimizing the risk of injury. Whether for athletic performance, daily activities, or rehabilitation, a well-rounded approach to training and maintenance is key to achieving and sustaining optimal arm mobility.
Frequently asked questions
The primary muscle responsible for arm abduction is the deltoid muscle, specifically the middle deltoid fibers.
Arm abduction is the movement of raising the arm away from the body in the frontal plane, and it typically involves a range of motion from 0 to 180 degrees, with 0 degrees being the arm resting at the side and 180 degrees being the arm raised directly overhead.
Yes, in addition to the deltoid, the supraspinatus muscle (one of the rotator cuff muscles) also assists in initiating arm abduction, particularly in the first 15 degrees of the movement.
Exercises that target the deltoid and supraspinatus muscles include lateral raises, shoulder presses, upright rows, and cable lateral raises, all of which help strengthen the muscles involved in arm abduction.