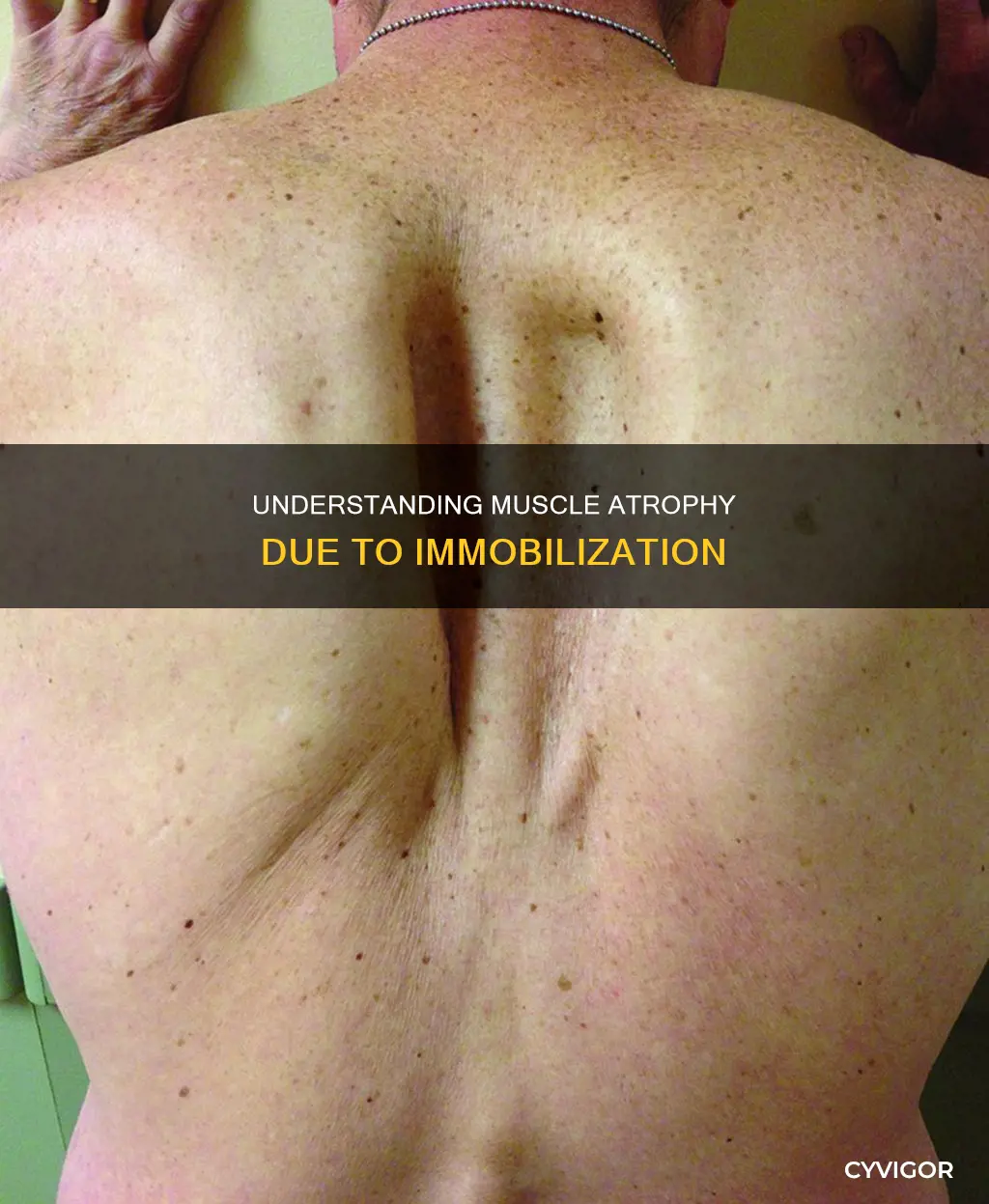
Immobilisation of the limbs can cause rapid muscle atrophy, resulting in a loss of muscle mass and strength. This is a common consequence of sports injuries. The molecular regulation of muscle mass in the rehabilitation of immobilisation-induced atrophy is not well understood, although muscle mass is known to be regulated by the relative rates of protein synthesis and protein breakdown.
| Characteristics | Values |
|---|---|
| Cause | Immobilisation or disuse after sports injuries |
| Response | Loss of muscle mass and strength |
| Recovery | Requires appropriate rehabilitation to restore normal function |
| Molecular regulation | Sparsely studied |
| Muscle mass | Regulated by the relative rates of protein synthesis and protein breakdown |
| Protein synthesis | Reduced |
| Protein breakdown | Increased |
| Autophagic activities | Play an important role in the early stages of muscular atrophy |
| Oxygen supply | May be impaired |
| Myoglobin content | Increased |
| Mitochondrial function | Lost during the first days of disuse |
| Connective tissue | Increased in atrophic muscle and surrounding periarticular tissue |
Explore related products






What You'll Learn
- Sports injuries can cause immobilisation and muscle atrophy
- Rehabilitation is required to restore normal function after muscle atrophy
- Molecular regulation of muscle mass is understudied in the rehabilitation of immobilisation-induced muscle atrophy
- The rate of protein synthesis is reduced in atrophic muscle
- The oxygen supply to a disused muscle may be impaired
![]()
Sports injuries can cause immobilisation and muscle atrophy
Muscle atrophy occurs when the rate of protein synthesis is reduced and the rate of protein breakdown is increased. The oxygen supply to the muscle may also be impaired, and the complete loss of mitochondrial function during the first few days of disuse may be significant. The amount of connective tissue is increased in atrophic muscle, which may lead to a vicious cycle of musculoskeletal degeneration.
The molecular regulation of muscle mass in the rehabilitation of immobilisation-induced muscle atrophy is not well understood. However, muscle mass is regulated by the relative rates of protein synthesis and protein breakdown, and the key Akt, mammalian target of rapamycin (mTOR), glycogen synthase kinase 3β (GSK3β) and Forkhead box O (FOXO) signalling pathways. Akt is activated by insulin and insulin-like growth factor 1 (IGF-1), and the forced transgenic or pharmacologic induction of Akt in vivo or in vitro is sufficient to cause dramatic muscle hypertrophy and inhibit atrophy.
An almost complete recovery from atrophy is possible, but the recovery phase is often much longer than the immobilisation period. Appropriate rehabilitation is required to ensure the restoration of normal function.
Muscle Decay: Understanding Rapid Loss and Prevention
You may want to see also
Explore related products






![]()
Rehabilitation is required to restore normal function after muscle atrophy
Limb immobilisation causes a rapid loss of muscle mass and strength, which requires rehabilitation to restore normal function. The molecular regulation of muscle mass in the rehabilitation of immobilisation-induced atrophy is understudied, but muscle mass is regulated by the relative rates of protein synthesis and protein breakdown. The Akt, mammalian target of rapamycin (mTOR), glycogen synthase kinase 3β (GSK3β) and Forkhead box O (FOXO) signalling pathways are key to this process.
Akt is activated by insulin and insulin-like growth factor 1 (IGF-1), and the forced transgenic or pharmacologic induction of Akt in vivo or in vitro is sufficient to cause dramatic muscle hypertrophy and inhibit atrophy. An almost complete recovery from atrophy is possible, but the recovery phase is often much longer than the total immobilisation period.
To restore normal function, rehabilitation should include physiotherapy and protein/carbohydrate supplementation.
Muscle Memory: How Do Muscles Retain Information?
You may want to see also
Explore related products






![]()
Molecular regulation of muscle mass is understudied in the rehabilitation of immobilisation-induced muscle atrophy
Immobilisation-induced muscle atrophy is a common consequence of sports injuries. Limb immobilisation causes a rapid loss of muscle mass and strength, requiring appropriate rehabilitation to restore normal function. Despite the importance of appropriate recovery, the rehabilitation of muscle mass and function following immobilisation is understudied. While knowledge of muscle mass signalling with immobilisation has increased in recent years, there is a paucity of studies on the molecular regulation of muscle mass in the rehabilitation of immobilisation-induced muscle atrophy.
Muscle mass is regulated by the relative rates of protein synthesis and protein breakdown. The molecular regulation of this includes the key Akt, mammalian target of rapamycin (mTOR), glycogen synthase kinase 3β (GSK3β) and Forkhead box O (FOXO) signalling pathways. Akt is activated by insulin and insulin-like growth factor 1 (IGF-1). The forced transgenic or pharmacologic induction of Akt in vivo or in vitro is sufficient to cause dramatic muscle hypertrophy and inhibit atrophy.
To investigate the molecular regulation of muscle mass in the rehabilitation of immobilisation-induced muscle atrophy, two separate studies were conducted. In the first study, the lower limb was immobilised for 2 weeks, followed by in-house hospital standard physiotherapy rehabilitation. In the second study, an intervention was conducted using the same 2-week immobilisation protocol, during which protein/carbohydrate supplementation was given.
The results of these studies provide valuable insights into the molecular regulation of muscle mass during rehabilitation. However, further research is needed to fully understand the complex processes involved in muscle atrophy and recovery. By gaining a deeper understanding of the molecular mechanisms underlying muscle atrophy and rehabilitation, we can develop more effective strategies to prevent and treat this common condition, improving patient outcomes and quality of life.
The Ciliary Muscle: How Does It Affect Your Vision?
You may want to see also
Explore related products





![]()
The rate of protein synthesis is reduced in atrophic muscle
Immobilisation of the limbs can cause a rapid loss of muscle mass and strength. This is known as muscular atrophy. It is a common consequence of sports injuries and requires appropriate rehabilitation to restore normal function.
Muscle mass is regulated by the relative rates of protein synthesis and protein breakdown. In atrophic muscle, the rate of protein synthesis is reduced, and the rate of protein breakdown is increased. This is known as a catabolic metabolism. The oxygen supply to the disused muscle may also be impaired, and the complete loss of mitochondrial function during the first few days of disuse may be significant.
The molecular regulation of muscle mass in the rehabilitation of immobilisation-induced muscle atrophy is not well understood. However, it is known that the Akt, mammalian target of rapamycin (mTOR), glycogen synthase kinase 3β (GSK3β) and Forkhead box O (FOXO) signalling pathways are involved. Akt is activated by insulin and insulin-like growth factor 1 (IGF-1), and its induction can cause dramatic muscle hypertrophy and inhibit atrophy.
Earthworms' Muscular Movement: Understanding Their Unique Locomotion
You may want to see also
Explore related products






![]()
The oxygen supply to a disused muscle may be impaired
Immobilisation or disuse after sports injuries can cause muscle atrophy. This is characterised by a catabolic metabolism, where the rate of protein synthesis is reduced and the rate of protein breakdown is increased. The oxygen supply to a disused muscle may be impaired, although myoglobin content is increased in atrophic muscle. The complete loss of mitochondrial function during the first few days of disuse may be of aetiological importance. The amount of connective tissue is increased in atrophic muscle and surrounding periarticular tissue, which may lead to a vicious circle of musculoskeletal degeneration.
Limb immobilisation causes a rapid loss of muscle mass and strength that requires appropriate rehabilitation to ensure restoration of normal function. The molecular regulation in the rehabilitation of immobilisation-induced muscle atrophy is only sparsely studied. Muscle mass is regulated by the relative rates of protein synthesis and protein breakdown, and the molecular regulation of this includes the key Akt, mammalian target of rapamycin (mTOR), glycogen synthase kinase 3β (GSK3β) and Forkhead box O (FOXO) signalling pathways. Akt is activated by insulin and insulin-like growth factor 1 (IGF-1), and the forced transgenic or pharmacologic induction of Akt in vivo or in vitro is sufficient to cause dramatic muscle hypertrophy and inhibit atrophy.
Understanding Muscle Contractures: Causes and Mechanisms
You may want to see also
Frequently asked questions
Immobilization atrophy is the loss of muscle mass and strength due to immobilization or disuse after sports injuries.
Immobilization atrophy is caused by a rapid loss of muscle mass and strength. This can be due to a lack of use or immobilization of a limb.
Immobilization atrophy can lead to a complete loss of mitochondrial function and an increase in connective tissue, which may result in a vicious cycle of musculoskeletal degeneration.
The most evident response to immobilization atrophy is strength loss. Other signs include reduced protein synthesis and increased protein breakdown.
Treatment for immobilization atrophy includes appropriate rehabilitation to ensure the restoration of normal function. This may include physiotherapy or protein/carbohydrate supplementation.































